This month’s ASAT feature comes to us from Judith Ursitti. To learn more about ASAT, please visit their website at www.asatonline.org. You can also sign up for ASAT’s free newsletter, Science in Autism Treatment, and like them on Facebook!
Judith Ursitti, Mother of Jack
I love this young man with all of my heart. I worry about his future. He has so much to offer this world. But frequently, I read things that seem like they deny the realities of valuable humans like him.
He’s not a savant. He doesn’t type. He gets up in the morning and gets ready for school. He works hard every day, striving for connection and independence, supported by a team of loving therapists.
Speech, OT, PT, ABA,… All of it aimed at empowering him. He runs and swims after school. Exercise is such great medicine. He’s not into TV or movies, really. He spends no time on the internet. He loves listening to music on his iPad. Lately, it’s been Katy Perry and Kanye.
He was diagnosed with autism at age two. He was diagnosed with a severe intellectual disability at nine. A diagnosis of OCD came a little later. This combination of alphabet soup brings a lot of pain and struggle. He’s hurt himself. He’s hurt me. It can be hard.
He loves and is loved. He likes to swing as high as the swing will go. He loves to go to the store. He loves to go to Outback Steakhouse and eat wings. He loves his sister and is sometimes annoyed with her. He likes to hang close. He also likes to be left alone.
He hums and rocks and paces. He laughs. He enjoys looking in the mirror and making goofy faces. He screams loudly over and over and laughs and laughs and laughs. He is authentic. Refreshingly so.
He is not the prom king. He is not represented in research or the media very much. It’s very hard for researchers to include people like him in their work. His sensory challenges, his inability to read or write or speak leave him on the periphery of autistic representation.
I have many autistic friends with various profiles. They are some of my favorite people. Truly. The truth is his severity makes him really different than them. I’m not even certain that the shared diagnosis is accurate. But hey, I’m not a scientist.
But I do think this is such a compelling reason to work really hard to conduct research for people like him. Individualized supports and services can really help human beings like him.
What’s the point of my rambling? Please just know that when you hear the word autism, or you read something by autistic authors representing the autism community, it’s generally not inclusive of people like my son. This needs to change. His experience matters.
He and so many others like him need inclusion, acceptance, and support, particularly from their own community. They desperately need research to provide answers and to improve their quality of life.
The ongoing balance of joy and pain is part of the human experience. But his version of it weighs heavily on him. He deserves peace. Please don’t forget about people like him.
About the Author:
Judith Ursitti is Vice President of Government Affairs for the Council of Autism Service Providers (CASP). A CPA by training, she spent a decade working in tax accounting. She became immersed in the world of autism advocacy when her son, Jack, was diagnosed at age 2. Since his diagnosis, she has worked on the passage, implementation, and enforcement of autism-related legislation nationwide. She worked for Autism Speaks as their director of state government affairs for over a decade. She has served on the Massachusetts Autism Commission, where she co-chaired the Commission’s 14-22/Employment Subcommittee. She also serves as the public policy chair of the National Council on Severe Autism and is the co-founder of the Profound Autism Alliance. She frequently writes about autism advocacy and her experiences parenting a son with profound autism.with autism.
Citation for this article:
Ursitti, J. (2022). Jack matters, too: A mother’s perspective on her son’s place in the autism community. Science in Autism Treatment, 19(7).
Setting IEP goals for autistic learners can be incredibly difficult, especially when you’re working with emerging communicators. At the beginning of my career, assessment tools were limited and I found out along the way the goals I set for my students were unclear and hard to measure. Assessment, collaboration and functional goals are all important pieces of the puzzle for setting up your student and the therapy for success.
Standardized tests are commonly used in the classroom, but they are so tricky because they often do not give us the snapshot of skills we need for autistic learners. Assessment tools I recommend if you have access are the VB-MAPP and the Functional Communication Profile. If you don’t yet have access or need to start on a more basic level, I like to look for specific early learner skills. These are those small basic skills that lead to learning bigger skills and tasks. These are measurable communication skills that start in even really young learners such as labeling, verbal imitation, intraverbal skills like filling in the blank, matching, and group listening.
When you have brought all the pieces together, it’s time to set the vision for their communication programming. I have 5 questions for you to ask as a part of my practical and systematic approach to establishing functional goals for your autistic learner.
What behavior are we targeting?
Is it appropriate for our client?
How is this goal specific?
Is the goal observable?
What does mastery look like?
No matter the skill level, the age, or the context of your therapy practice, this approach will help you consider all the important pieces behind each goal. If you’re a parent, this can help you know what questions to ask your therapist and IEP team to ensure the right goals are being observed and measured for your child. As a part of this episode, I have included a downloadable link for my IEP Goal Bank, be sure to check it out as you work with your team and parents to set specific, actionable IEP goals for your autistic learners.
Rose Griffin, SLP, BCBA is dedicated to helping SLPs and other professionals provide systematic language instruction with ease. Working with students with autism and other complex communication disorders can be challenging. Rose has dedicated herself to helping by providing professional development and real life examples of what she does in her daily practice. See her podcast, blog, and collaboration opportunities at www.abaspeech.org
By: May Chriseline Beaubrun, MEd, BCBA (Brett DiNovi & Associates)
Prior to offering some global suggestions, I wanted to highlight some of the available research that explains of the unique experiences of Black families of children with autism. Although autism does not discriminate (across race, ethnicity, culture, socio-economic status, etc.), diagnosis, access to resources, treatment options, and culturally competent care can vary vastly for Black families with children with autism (Čolić et al., 2021). For example, Black children with intellectual disabilities receive an autism diagnosis an average of six months later than comparable white children (Dryden, 2020). Mandell et al. (2002) found that Black parents on average made three times more visits to doctors to obtain an autism spectrum disorder (ASD) diagnosis than their white counterparts. Dyer (2018) found that Black parents had seen multiple specialists before their children finally received a diagnosis. These setbacks in diagnosing Black children translate into a delay in skill acquisition, reduced access to early intervention, and an increased risk of challenging behaviors (Čolić et al., 2021). Also, an estimated 47 percent of Black autistic children also have an intellectual disability, compared to 27 percent of white children (Dattaro, 2020); and these delays in autism diagnosis may be a contributing factor in the high rate of intellectual disability among Black autistic children in the United States.
Constantino et al. (2020) examined the experiences of Black families affected by ASD in the United States. The researchers found that Black families were concerned about a child’s development, language, or behavior. The study consisted of interviews of 584 parents of Black children with autism. The authors compiled timelines of the Black families’ experiences, including the developmental outcomes of the autistic children and their siblings. The following sections describe the two most important findings:
Timeline To Diagnosis: The authors found a three-year delay in diagnosis. The parents first noted concerns about their child’s development around 23 months of age; told a professional six months later; and did not receive an autism diagnosis until their child was over 5 years old.
Timeline to Treatment: More than a third of the families reported long wait times to see a professional; 14 percent made at least six visits to specialists before their child was diagnosed. Nearly a third said that a lack of available professionals contributed to the diagnostic delay.
Additional Barriers: More critical than the timing of diagnosis is educating Black families about the signs of ASD. This means that due to the lack of educational information and programs for Black parents in their community, they had to learn about ASD by themselves, very often through the internet (Burkett et al., 2015; Lovelace et al., 2018). The internet is useful for accessing quick information, such as directions, office hours, etc., but can be dangerous when researching treatment options (see this article for more information). Additionally, the disparities continue beyond the time of diagnosis to access to intervention services (Constantino et al., 2020). For example, in the Čolić et al. (2021) article, Black parents reported that practitioners would assume that they did not have private insurance. When assuming someone does not have insurance, they may not be offered the benefits of treatment options that are available.. Also, as reported in Čolić et al. (2021), community-based instruction was often not offered in the belief that their neighborhood was dangerous and violent. Beyond getting a diagnosis, these confounding variables continue to impact Black families’ ability to access services.
Intellectual Disability Disproportionality – Disproportionality refers to a situation in which a particular group (e.g., racial, ethnic, etc.) are represented at a higher or lower percentage than their percentage in the general population. Although the diagnostic prevalence of autism is approximately the same across races (Mandell et al., 2009), there is a disproportionality of Black children who have a diagnosis of autism and have an intellectual disability. Similar to the findings of Dattaro (2020), the U.S. Centers for Disease Control and Prevention, show that 22% of white children with autism also have an intellectual disability but among African American children, the rate of intellectual disability in those with autism is over 44% (Dryden, 2020).
Poverty – Poverty which disproportionately affects Black families in the U.S, is associated with worse cognitive outcomes (Constantino, 2020). However, there are no links between the autistic children’s intelligence quotient (IQ) and their family’s income or parents’ education, meaning the increased prevalence of intellectual disability among Black autistic children cannot be attributed to poverty (Sohn, 2020).
Quality of Treatment: In the Magaña, Parish, and Son (2015) article, data from the 2005-2006 and 2009-2010 National Survey of Children with Special Health Care Needs were analyzed. The results indicated that racial and ethnic disparities in the quality of provider interactions were significant in both the 2005-2006 and 2009-2010 surveys, and were found to be unchanged over time. More so, these racial and ethnic disparities in healthcare quality were found to be unchanged over time. Black families were less likely than white and Latino families to feel that their provider helped them feel like a partner. They were also less likely to feel that the provider spent enough time with them; that the provider was sensitive to their family’s values; and that the provider listened to them. In my opinion, this is still a relevant issue and remains to be unchanged.
I hope I was successful sharing some of the recent research that shines a light on the myriad challenges facing Black families. I would like to now turn our attention to the final part of your question: how can myself and my colleagues better meet the needs of Black families I serve? Čolić et al (2021) identify four main areas where ABA practitioners should be especially sensitive to move towards culturally responsive ABA practice (a) build knowledge about Black cultural values, (b) show care and strengthen partnerships, (c) create culturally relevant interventions, and (d) be aware of one’s own prejudice and cultural values.
Build Knowledge about Black Cultural Values: During the initial intake and throughout the treatment, ABA practitioners, like yourself, can learn about the Black families’ culture, such as family dynamics, religious and spiritual beliefs, self-care, etc. and incorporate these considerations into treatment planning. Families should be included in the process which in term will lead to improved outcomes and program efficacy (Mathur & Rodriguez, 2021).
Show Care and Strengthen Partnerships: ABA practitioners must recognize the potential barriers Black families may have had to overcome prior to even requesting and accessing your services. Training on cultural diversity and cultural humility is needed to provide culturally responsive services. The families should feel comfortable advocating for changes to programs without feeling judged (Mathur & Rodriguez, 2021).
Create Culturally Relevant Interventions: When developing and implementing treatment goals, ABA practitioners should increase cultural humility. For example, when creating materials such as icons and pictures for communication, rule cards, visual cues, etc. the skin tone should represent that of the client, including a Black individual. When creating classroom rules and expectations, consider culturally responsive behavior management so that all students with equitable opportunities for learning. For example, use proactive language that is clear and reflects the student and the family voice.
Be Aware of One’s Own Prejudice and Cultural Values: ABA practitioners should recognize the impact that implicit bias and racism have on the efficacy and efficiency of behavioral analytic support services (Mathur & Rodriguez, 2021). Training in cultural humility should also include ABA practitioners recognizing their own implicit bias. Fong et al. (2016) illustrated how assumptions based on culture can impact a behavior analyst’s effectiveness with families of diverse backgrounds. Rather than make assumpations, seek sonculatation and supervision as needed. Treating one black family makes a practioner experienced in treating with one black family. For example, using a teaching set of community helpers who are all white males contributes to white supremacy.
Addressing the issues in the timing of diagnosis and the quality and quantity of treatment may help resolve disproportionately of Black children who have a diagnosis of autism and have an intellectual disability. I remain concerned about the implicit bias of providers that goes unchallenged, and that Black families will continue to feel unheard and not receive the same type of treatment as their white and Latino counterparts. As a BCBA, I am advocating for culturally responsive ABA practice.
References
Burkett, K., Morris, E., Manning-Courtney, P., Anthony, J., & Shambley-Ebron, D. (2015). African American families on autism diagnosis and treatment: The influence of culture. Journal of Autism and Developmental Disorders, 45(10), 3244–3254. https://doi.org/10.1007/s10803-015-2482-x.
Constantino, J. N., Abbacchi, A. M., Saulnier, C., Klaiman, C., Mandell, D. S., Zhang, Y., … & Geschwind, D. H. (2020). Timing of the diagnosis of autism in African American children. Pediatrics, 146(3).
Fong, E. H., Catagnus, R. M., Brodhead, M. T., Quigley, S., & Field, S. (2016). Developing the cultural awareness skills of behavior analysts. Behavior Analysis in Practice, 9(1), 84-94. https://doi.org/10.1007/s40617-016-0111-6.
Lovelace, T. S., Tamayo, S., & Robertson, R. E. (2018). Experiences of African American mothers of sons with autism spectrum disorder: Lessons for improving service delivery. Education and Training in Autism and Developmental Disabilities, 53(1), 3-16.
Mandell, D. S., Wiggins, L. D., Carpenter, L. A., Daniels, J., DiGuiseppi, C., Durkin, M. S., Giarelli, E., Morrier, M. J., Nicholas, J. S., Pinto-Martin, J. A., Shattuck, P. T., Thomas, K. C., Yeargin-Allsopp, M., & Kirby, R. S. (2009). Racial/ethnic disparities in the identification of children with autism spectrum disorders. American Journal of Public Health, 99(3), 493-498. https://doi.org/10.2105/AJPH.2007.131243
Magaña, S., Parish, S. L., & Son, E. (2015). Have racial and ethnic disparities in the quality of health care relationships changed for children with developmental disabilities and ASD?. American Journal on Intellectual and Developmental Disabilities, 120(6), 504-513.
Mathur, S. K., & Rodriguez, K. A. (2021). Cultural Responsiveness Curriculum for behavior analysts: A meaningful step toward social justice. Behavior Analysis in Practice, 1-9.
Beaubrun, M (2022). Clinical Corner: Understanding the needs of Black families of children with autism. Science in Autism Treatment, 19(4)
Author Bio: May Chriseline Beaubrun has been a Board Certified Behavior Analyst for over 10 years. She is currently the Director of Diversity & Training at Brett DiNovi & Associates. She has worked with children and adults with various cognitive, developmental, and physical disabilities in a variety of settings (e.g., clinic, hospital, home, school). She has completed program evaluations; developed skill acquisition programs to teach academic areas, cognitive functioning, social skills, language and communication, and adaptive skills; provided parent training; conducted functional behavior assessments (FBA); developed Behavior Intervention Plans (BIP), program evaluations and provided staff training to various levels of professionals. May has presented at the annual Autism New Jersey convention (formerly Center for Outreach and Services for the Autism Community) as well as Association for Behavior Analysis International, New Jersey Association for Behavior Analysis, and California Association for Behavior Analysis. May also was an adjunct professor at Philadelphia College of Osteopathic Medicine. May contributed a chapter to the text, A Scientific Framework for Compassion and Social Justice, on behavior analysis and urban planning. May’s areas of interest include cultural responsiveness and social justice.
Hey, it’s still the middle of Summer! Why are we talking about back to school already? Put down that pumpkin spice and get in the pool!
But seriously . . . like it or not, back to school is coming. Some students look forward to returning to school with anticipation, and some with dread. Some students who receive special education services attend school year-round. Even for these students, back-to-school may be an adjustment because the summer session may be characterized by shorter days, more recreational activities, different staff, and end a good few weeks before school restarts for the academic year.
For all children, it’s a good idea to start anticipating going back to school with some time for adjustment and planning. For students with special needs, this is especially important, as changes can be challenging. Here are some ideas for helping to ease that transition:
Talk about school and highlight the fun and exciting things they will get to do. Remember what was most reinforcing at school for your child last year, and help them to remember that, too. Did they love PE or music or art? Are they especially talented in math or writing? Do they have certain friends they like to play with at recess? Is the cafeteria pizza their absolute favorite? Is the walk to and from school something they enjoy?
Provide information about the coming year as you are able to. If your child will be starting school in a new building, make arrangements to visit the building a few times over the summer. Most schools will have these visit days or orientations arranged for all students, but you may be able to request an extra visit or two for a child who would benefit from some additional exposure.
When you make those visits, take some pictures and use them to develop a book or poster with your child that they can refer to as the summer progresses. Don’t just refer to the pictures if your child expresses anxiety or disappointment about school starting, but as a regular activity to build familiarity and (hopefully) anticipation.
Pay attention to your family sleep schedule. Sometimes the summer schedule can get a little loose, which may be great for everyone. We can all benefit from sleeping on our own natural schedule, but if that natural schedule departs in a big way from what will be needed during the school year you will want to start to gradually shift it back. To make the change less abrupt, in the weeks before school starts again, start to wake your child a bit earlier every day and get them to bed a bit earlier each night.
If your child is always an early waker, you might want to take advantage of a more relaxed summer schedule to focus on building independence in the morning routines. During the busy school year it can be challenging to take the time to let your child learn to do things independently, but summer is a great time to let them dress themselves, brush their own hair, and do other self-care tasks with your supervision.
Consider the routines that make your school-year mornings work well, and continue to practice them during less-stressful summer mornings. Keeping a reasonably structured routine throughout the summer, or reintroducing it a few weeks before school starts, can help everyone to adjust to the return to school more smoothly.
If possible, connect with parents of some of your child’s classmates and see if you can get them together over the summer. If social skills are difficult for your child, keep these playdates short and sweet. Try meeting up in enjoyable locations like the park or beach, and letting kids parallel play so that they are used to seeing each other. Pair these little gatherings with favorite snacks, fun activities that can be done together or alone (bubbles, sidewalk chalk, play-doh, jumping through a sprinkler), and remind the children that they will be seeing each other and playing more together when school starts.
For some children, school represents a return to certain demands that may not be present during the summer. If your child has sensitivities around clothing or food, you may be able to accommodate these more when they are not in school. While this is absolutely fine to do, it can be difficult if they need to abruptly shift back to different expectations when school starts again. Children who love to stay in their pajamas or bathing suits might be unhappy about school clothes, or those who get used to a hot, home-cooked lunch might not appreciate going back to sandwiches. Keeping some of these expectations part of the summer rotation can ease that stress. To whatever extent it feels comfortable and fair for your child and your family, continued exposure to school-year conventions are going to make the return to school easier for everyone.
We can all remember that going back to school is both exciting and challenging for everyone. In addition to cheering your child on as they return to a new school year and possible new challenges and triumphs, it’s equally important to be empathetic about disappointment that summer vacation is ending, and anxieties about upcoming changes. Compassionately addressing your child’s reactions to returning to school, whatever they may be, includes listening, understanding, and helping. What this looks like will be different for each child, but as a parent you have the knowledge of your unique child’s needs and strengths to provide compassionate support.
About the Author:
Dana Reinecke, Ph.D., BCBA-D is a New York State Licensed Psychologist and Licensed Behavior Analyst (LBA). Dana is an Assistant Program Director in the Applied Behavior Analysis department at Capella University, overseeing the PhD in Behavior Analysis program and mentoring doctoral learners. She is also co-owner of SupervisorABA, an online platform for BACB supervision curriculum and documentation. Dana has provided training and consultation to school districts, private schools, agencies, and families for individuals with disabilities. She has published her research in peer-reviewed journals, written chapters in published books, and co-edited books on ABA and autism. Current areas of research include use of technology to support students with and without disabilities, self-management training of college students with disabilities, and online teaching strategies for effective college and graduate education. Dana is a Past President of the New York State Association for Behavior Analysis (NYSABA).
Consider the different types of technology we use in our everyday lives. For example, most individuals use cell phones and computers daily. But did you know that many technology features we commonly use were initially designed for individuals with disabilities? These are called mainstream derivatives of assistive technology (AT). Take your cell phone, for example. Texting was originally intended for people with hearing challenges, and screen enlargement was initially designed for those with vision problems. As the demand for technology has increased, many AT features have become standard for all users.
Individuals with disabilities have the right to access environments that are available to all people. Accommodations are changes to conditions that provide access to the environment. AT devices are examples of accommodations that may be necessary for individuals with disabilities to allow them to overcome or circumvent barriers to their learning and living environments.
AT is defined by the Individuals with Disabilities Education Improvement Act (IDEA) in two parts: AT Technology and AT Devices. AT identifies the equipment that supports the individual in a specific area (e.g., communication, organization, activities of daily living). AT Services refer to the support or services needed to use the devices effectively. Both are integral parts of AT. For example, an individual cannot benefit from using a computer (AT device) if their caregivers and teachers have not taught them how to use it (AT Service).
The AT continuum consists of No-tech, Low-Tech, Mid-Tech, and High-Tech options designed to meet the needs of all learners:
• No-tech refers to unaided systems where an individual does not require anything beyond their body. Examples of No-Tech AT are vocalizations, verbalizations, eye gaze, or facial expressions.
• Low-Tech devices are generally comprised of materials that are easily obtainable, easy to use, low cost, and do not require a power source. Examples include graphic organizers, visual schedules, post-it notes, and manipulatives.
• Mid-tech devices, not used as often as low-tech or high-tech devices, generally require a power source. A simple switch, digital recorder, or adapted keyboard are examples of Mid-tech AT.
• High-Tech AT options are more complex, expensive to make or buy, and are usually programmable, such as a computer, iPad, AAC device, or electric wheelchair. Currently, much of AT is computerized and requires training to be used effectively.
Which type of AT is right for your child? Consider each level of AT to determine the best and most practical option for your child in their specific environment. The goal is always to foster independence. Ask, “Can your child perform the skill or task without AT?” If the answer is yes, then no AT is needed. If the answer is no, move through the continuum to find the technology that best supports their needs. Remember that high-tech devices are not necessarily superior to low and mid-tech devices. They tend to be costly and are not as easy to modify. A low-tech device is designed with simplicity and can provide users with flexibility and independence. For example, a student may benefit from using a low-tech pencil grip or a finger-spacing tool for writing rather than a high-tech mapping software or smartpen tool. Similarly, a student with organizational challenges and working memory issues may become overwhelmed with a high-tech application found on an iPad or tablet and benefit from a basic, teacher-constructed graphic organizer. In contrast, there are times when a high-tech device is the best AT choice for the learner. For example, a child may require an AAC device or application to communicate and access language.
When choosing a device, consider your child’s individual needs, the device’s practicality, and the user’s preferences and interests. Your child can benefit from using AT as it allows them to build strengths and address challenges. Remember that AT is most effective when learners are excited and motivated to incorporate its use into their learning repertoire.
Does your child have big reactions when you tell them no? Is the word no sometimes or often a trigger for your child leading to all kinds of problem behaviors?
We have to tell our kids no. No- do not run into traffic. No- do not touch a hot stove. And no- do not stray outside of the boundaries we have set as your parents. Take all the freedom you want within these boundaries, but no don’t stray.
But are there other ways to get your point across without the word no itself. If we can avoid the word that triggers the big reactions, maybe, just maybe we can avoid those meltdowns completely and spend our efforts focused on teaching and building up the good stuff.
What are some other ways to say no?
Not right now.
You can do (this) instead.
Maybe another time.
We have to do ____ right now.
Sure you can (do/have) that after you do (this) first.
Please do (this) instead.
I wish we could, but…
I’m afraid not.
I don’t think so.
Bummer! Not right now.
That’s not possible right now.
What a great idea, but not right now.
If you are telling your child to stop doing something or no, don’t do that action, try flipping your phrasing to what they CAN do instead.
From this
To that
No running.
Walk.
No jumping on the couch.
Sit on the couch.
No candy before dinner.
You can have candy at or after dinner.
No yelling.
Use your inside voice.
No grabbing.
Ask your sibling for a turn with the toy.
If the word no has been conditioned to cause an over the top reaction from your child, stop using the word no. Use other alternatives that get the same point across.
Whenever you find yourself about to say no, try to reframe it to tell your child what they can do or have instead. Give choices as much as possible.
Can I have some candy?
You can have some grapes or a banana.
Can we go to the park?
We can play trains or lego at home right now.
Child is running around the house.
You can walk in the house or run in the backyard.
No means no. But other wording also means no and is associated with a learning history of problem behavior. If something super simple like changing up our wording can help us move more quickly past the problem behavior- why not try it?! We want to spend our time and energy on teaching the more appropriate ways to communicate wants and needs instead of just dealing with problems.
Leanne Page, MEd, BCBA, is the author of Parenting with Science: Behavior Analysis Saves Mom’s Sanity. As a Behavior Analyst and a mom of two little girls, she wanted to share behavior analysis with a population who could really use it- parents!
Leanne has worked with children with disabilities for over 10 years. She earned both her Bachelor’s and Master’s degrees from Texas A&M University. She also completed ABA coursework through the University of North Texas before earning her BCBA certification in 2011. Leanne has worked as a special educator of both elementary and high school self-contained, inclusion, general education, and resource settings.
Leanne also has managed a center providing ABA services to children in 1:1 and small group settings. She has extensive experience in school and teacher training, therapist training, parent training, and providing direct services to children and families in a center-based or in-home therapy setting.
Leanne is now located in Dallas, Texas and is available for: distance BCBA and BCaBA supervision, parent training, speaking opportunities, and consultation. She can be reached via Facebook or at Lpagebcba@gmail.com.
By: Catherine L. McHugh, MA, BCBA, LBA and Thomas Zane, PhD, BCBA-D Department of Applied Behavioral Science, University of Kansas
Historically, teaching a communicative repertoire to children or individuals with autism spectrum disorder (ASD) and intellectual and developmental disabilities (IDD) focused on vocal verbal speech and modeling a speech sound with the hopes of the individual being able to imitate that sound (Charlop-Christy et al., 2002). However, prompting vocal verbal behavior is limited in comparison to a physical motor movement. Unless the individual has the ability to imitate, teaching speech sounds may be difficult (Bondy & Frost, 2001). Sign language is one potentially excellent option for teaching an alternative modality for communication. However, it also requires the individual to be able to attend to and imitate, as well as discriminate, very fine motor movements (Shwartz et al., 1998). For individuals with ASD and IDD, this may be a skill deficit making it very difficult to learn complex language. Therefore, Andy Bondy and Lori Frost turned their attention to exploring different modalities of communication that may better lend themselves to prompting and therefore result in greater contact with reinforcers. At the time of the development of Picture Exchange Communication System (PECS; Bondy & Frost, 2001), picture pointing was emerging as a form of communication; however, the individual may point to and cover the picture (i.e., preventing the communication partner from being able to see the image selected). Or they may touch the picture when no one is attending to them and therefore miss an opportunity for reinforcement resulting in possible extinction of the behavior. Bondy and Frost (2001) wanted to focus more on the communication exchange that occurs in language, so they developed a communication modality that teaches the individual to select a picture, pick it up, and place it in the hand of the communicative partner. This allows the teacher or caregiver to use physical prompts for communication and reduce the number of required prerequisite skills of the learner.
According to the seminal article by Bondy and Frost (2001), there are six steps of teaching PECS. The first focuses on the physical exchange and how to communicate. It teaches the learner the basic exchange of communication (i.e., expressing an idea to another person via the exchange of a symbol). Once the individual masters the exchange, the second step is referred to as the distance and persistence phase. This phase tests the durability of the communicative response, focusing on increasing the distance and response effort of communication such that the learner may have to travel and recruit the attention of the partner in order to contact reinforcement, as well as travel in order to access the symbols themselves. The third phase focuses on discrimination between symbols such that as more pictures are added to their system, they are able to find and exchange the picture that corresponds to the item they want. The fourth phase involves increasing the mean length of utterance and using phrases such as “I want” or “I see”. This allows the learner to move from mands (i.e., requesting) to perhaps engaging in tacts (i.e., labeling) or intraverbals (i.e., responding to questions). Phase five teaches the learner how to use PECS to answer questions and finally, phase six teaches commenting. As mentioned, not all phases need to be taught or mastered. Phase one is the building block for the remaining phases, but teaching the fundamental phase 1 exchange can have major implications for communication and other areas of the individual’s life. There are articles and manuals on how to use and teach PECS (e.g., Charlop-Christy et al., 2002; Conklin & Mayer, 2011; Frost, 2002; Paden et al., 2012; Schwartz et al., 1998), but the question remains, is there science behind PECS?
The existing research literature on PECS is vast and focuses on different phases and aspects of the system across populations with various skill sets and goals. Fortunately, researchers have produced several meta-analyses and review papers, so they will be summarized here.
For example, Preston and Carter (2009) reviewed the literature on PECS and found studies that utilized both randomized control trials (RCT) and single subject designs. The authors noted that, at the time, there had been only three experiments using RCTs and concluded that the methodology and data were insufficient for drawing any conclusions on the efficacy of PECS and encouraged future researchers to conduct more research in this area. However, Preston and Carter also noted that there was supporting evidence for PECS provided across the experiments that incorporated single subject research design methodologies. In conclusion, they found preliminary support for PECS as a communication modality for children and adults with ASD and IDD who have little or no vocal verbal language.
Sulzer-Azaroff et al. (2009) reviewed 34 peer-reviewed publications on PECS. This review included children and adult participants working with caregivers, teachers, and parents. Sulzer-Azaroff and colleagues reported that the results suggested that PECS was effective in teaching individuals who previously had no or limited functional communication, how to communicate. Most of these individuals learned new requests and some learned the more advanced phases in which they learned to describe things. When they reviewed articles that compared PECS to another modality, Sulzer-Azaroff et al. (2009) noted that the participants performed the same or better with PECS (e.g., Adkins & Axelrod, 2002). Overall, the results of this literature review further supported the use of PECS for teaching communication to non-speaking individuals.
Hart and Banda (2010) conducted a meta-analysis of the single subject research design studies on PECS. They reviewed 13 published studies and found that teaching PECS increased functional communication for all but 1 participant. They also noted some reasons why it might have been so successful for this population. First, the basic PECS procedure incorporates motivating operations (MO; Poling, Lotfizadeh, & Edwards, 2017) for teaching requests. The use of MOs presumes to increase the value of the reinforcer thereby increasing the likelihood of the individual engaging in the exchange in order to access the items. This contingency is very salient and likely a major reason why so many are able to acquire phase one of PECS so quickly. Therefore, PECS has the ability to teach someone abstract concepts using more salient stimuli and behaviors.
Schreibman and Stahmer (2014) conducted a randomized control comparison of the effects of verbal and pictorial communication on spoken language for children with autism. This study included 19 randomly assigned 2.5-year old’s who had a diagnosis of ASD that had fewer than 10 spoken words at the onset of the intervention. Participants in this study acquired about 90 spoken words on average after 6 months and about 120 spoken words after 9 months following intervention, showing strong evidence of the effectiveness of PECS.
According to these and more recent work on PECS, it appears that there is science to support the use of PECS for teaching communication to individuals with ASD and IDD across the lifespan. What is also interesting about PECS is some of the affected collateral behaviors (i.e., behaviors that were not directly targeted in the intervention) that are noted in these and other studies. First, there are some reports of vocalizations emerging while teaching PECS (e.g., Greenberg et al., 2014; Hart & Banda, 2010; Sulzer-Azaroff et al., 2009). For example, Greenberg et al. (2013) studied the amount and pattern of their participants’ vocalizations before and after PECS training. In study 1, the experimenters measured spontaneous vocalizations during and after PECS training. They saw an increase in vocalizations when compared to baseline. In study 2, participants who demonstrated limited vocalizations after study 1 were exposed to a procedure that included a time-delay prompt (i.e., waiting 3 seconds after the picture exchange to deliver the item to see if they would emit a vocalization) and verbal prompting procedures. Results of study 2 suggest that spontaneous vocalizations increased and occurred with every exchange. These results were quite promising and addressed the concern that if caregivers teach an individual to use PECS, they might not learn to vocalize. This does not seem to be the case. The emergence of vocalizations may be due to a variety of factors and is an empirical question that researchers should continue to study.
Another possible benefit of teaching PECS was reported by Hart and Banda (2010), who noted that in the studies they reviewed, there was a decrease in problem behavior for the participants who learned PECS. This is likely due to the fact that the individuals are learning functional communication skills. Functional communication training (FCT) is a procedure that teaches individuals a more appropriate way to request (i.e., communication rather and problem behavior) access to their reinforcers (Tiger et al., 2008). FCT can include a variety of communication modalities, but picture exchange is commonly used in the literature (e.g., Tiger et al., 2008). During FCT, the individual receives access to their reinforcer for a communicative response and no longer receives it for problem behavior. Therefore, they are taught a new way to get the things they need and want without engaging in problem behavior. One can also look at this from a response effort perspective. Communication is much less effort than engaging in physical aggression. Therefore, once PECS is acquired, the child may prefer this response that requires less effort and results in their preferred items.
Conclusions and Future Research
Numerous literature reviews and individual research studies provided evidence to strongly suggest that PECS can be considered an evidenced-based procedure. So, parents and caregivers can confidently use PECS to establish and shape communication in their children, with confidence that improvements are likely to be made. Furthermore, there are manuals that are both clear and comprehensive to guide the implementation of each step of the system.
Given that, continued research to establish whether or not PECS works seems unnecessary. Instead, researchers involved in studying this communication system could extend what is known about PECS along different variables and dimensions. For example, more research could be done on the extent of generalization and maintenance of PECS acquisition. Another area to address would be the preference of communication modality – that is, studying what influences an individual to select different communication systems, such as PECS, signs, or speech. Although some small n studies have been done on this (e.g., Tincani, 2004), it remains a very fruitful avenue to explore. Finally, it would be helpful to develop a more comprehensive literature based on the issue of whether the acquisition of PECS is responsible for a reduction in behavior problems and a spontaneous increase in spontaneous vocalizations.
The experimental research shows that PECS is an evidenced-based procedure. When working with individuals with communication impairments, PECS can be used to establish foundational or complex communication. Since communication deficits are one of the common symptoms of ASD, this particular procedure is a very welcomed and needed intervention approach.
About the Authors
Catherine McHugh, M.A., BCBA, LBA-KS is a doctoral student in Dr. Claudia Dozier’s lab at the University of Kansas in the Applied Behavioral Science Department. She a Board-Certified Behavior Analyst and a Licensed Behavior Analyst in the state of Kansas. Catherine completed her Masters of Applied Disability Studies and then a Masters of Arts with a focus in Applied Behavior Analysis at Brock University, St. Catharines, Ontario, Canada. She is the Vice President of the Graduate Student Organization for the Applied Behavioral Science Department at the University of Kansas. Catherine has worked with individuals with intellectual and developmental disabilities across the lifespan from children to older adults who engage in severe problem behavior.
Dr. Thomas Zane is a Professor of Practice and the Director of Online Programs in Behavior Analysis in the Department of Applied Behavioral Science at the University of Kansas. Dr. Zane earned his Bachelor’s and Master’s degree in psychology at Western Michigan University and his doctorate in Applied Behavior Analysis at West Virginia University. He has served as a Post-Doctorate Research Associate at the University of Massachusetts and as a Research Scientist at Johns Hopkins University Department of Psychiatry. Dr. Zane serves on the Executive Board of the Cambridge Center for Behavioral Studies, the international organization that represents the field of behavior analysis. He is also a member of the Scientific Council of the Organization of Autism Research, a group that funds innovative research in Autism Spectrum Disorders. Dr. Zane has been past President of the Ethics Special Interest Group of the International Association for Behavior Analysis. His research interests include online learning, evidenced-based practice in autism, and the philosophy of science and radical behaviorism. He is particularly interested in why some behavior analysts drift from the code and the importance of adhering to choosing scientifically-supported treatments in clinical and educational work.
References
Adkins, T., & Axelrod, S. (2002). Topography-versus selection-based responding: Comparison of mand acquisition in each modality. The Behavior Analyst Today, 2(3), 259–266. http://dx.doi.org/10.1037/h0099941
Charlop-Christy, M. H., Carpenter, M., Le, L., LeBlanc, L. A., & Kellet, Kristen. (2002). Using the Picture Exchange Communication System (PECS) with children with autism: Assessment of PECS acquisition, speech, social-communicative behavior, and problem behavior. Journal of Applied Behavior Analysis, 35(3), 213-231. https://doi.org/10.1901/jaba.2002.35-213
Conklin, C. G., & Mayer, G. R. (2011). Effects of implementing the Picture Exchange Communication System (PECS) with adults with developmental disabilities and severe communication deficits. Remedial and Special Education, 32(2), 155-166. https://doi.org/10.1177%2F0741932510361268
Frost, L., & Bondy, A. (2002). The Picture Exchange Communication System training manual. (2nd Ed.). Pyramid Educational Products.
Greenberg, A. L., Tomaino, M. E., & Charlop, M. H. (2013). Adapting the Picture Exchange Communication System to elicit vocalizations in children. Journal of Developmental and Physical Disabilities, 26(1), 35-51. http://dx.doi.org/10.1007/s10882-013-9344-2
Hart, S. L., & Banda, D. (2010). Picture Exchange Communication Systems with individuals with developmental disabilities: A meta-analysis of single subject studies. Remedial and Special Education, 31(6), 476-488. https://doi.org/10.1177/0741932509338354
Paden, A. R., Kodak, T., Fisher, W. W., Gawley-Bullington, E. M., & Bouxsein. (2012). Teaching children with autism to engage in peer-directed mands using a Picture Exchange Communication System. Journal of Applied Behavior Analysis, 45(2), 425-429. https://doi.org/10.1901/jaba.2012.45-425
Poling, A., Lotfizadeh, A., & Edwards, T. L. (2017) Predicting reinforcement: Utility of the motivating operations concept. Behavior Analyst, 40(1), 49-56. http://dx.doi.org/10.1007/s40614-017-0091-z
Preston, D., & Carter, M. (2009). A review of the efficacy of the Picture Exchange Communication System intervention. Journal of Autism and Developmental Disorders, 39(10), 1471-1486 . http://dx.doi.org/10.1007/s10803-009-0763-y
Tiger, J. H., Hanley, G. P., & Bruzek, J. (2008). Functional communication training: A review and practical guide. Behavior Analysis and Practice, 1(1), 16-23. https://doi.org/10.1007/BF03391716
Tincani, M. (2004). Comparing the Picture Exchange Communication System and sign language training for children with autism. Focus on Autism and Other Developmental Disabilities, 19(3), 152-163. http://dx.doi.org/10.1177/10883576040190030301
Schreibman, L., & Stahmer, A. C. (2014). A randomized trial comparison of the effects of verbal and pictorial naturalistic communication strategies on spoken language for young children with autism. Journal of Autism and Developmental Disabilities, 44(5). 1244-1251. http://doi.org/10.1007/s10803-013-1972-y
Schwartz, I. S., Garfinkle, A. N., & Bauer, J. (1998). The Picture Exchange Communication System: Communicative outcomes for young children with disabilities. Topics in Early Childhood Special Education, 18(3), 144-159. http://dx.doi.org/10.1177/027112149801800305
Sulzer-Azaroff, B., Hoffman, A. O., Horton, C. B., Bondy, A., & Frost, L. (2009). The Picture Exchange Communication System what do the data say?” Focus on Autism and Other Developmental Disabilities, 24(2), 89-103. https://doi.org/10.1177/1088357609332743
Citation for this article:
McHugh, C. L., & Zane, T. (2022). Picture Exchange Communication System: Is there science behind that? Science in Autism Treatment, 19(5).
By: Katie McKenna, MS, OTR/L (originally posted on The Autism Helper)
It is so hard to believe that summer is upon us! Summer can bring about many different experiences and emotions. On one hand, it can be exciting to take a break from the intense schedule of the school year. However, on the other hand, summer often brings less structure and routine, which can be hard for our learners. As I wrap up the school year, I like to provide my families with some therapeutic activity ideas that not only maintain or build skills throughout the summer but also are fun and easy to implement. Here are some of my tips for putting together a summer therapy home program!
1. Embrace the Outdoors
Summer is the best time to truly embrace outdoor activities. Kids NEED to be active. Check out my blog post here about why outdoor play is so vital. Additionally, many summer activities that families naturally do may include amazing outdoor motor and sensory experiences, such as swimming, going to the beach, hiking and bike riding. Even just playing at the playground can be so beneficial – check out this post for more! When recommending summer activities for families, I always include outdoor play ideas as they tend to be easy to setup and free or low cost, but full of amazing opportunities for students.
2. Encourage Hands On Activities
Early in my career, I used to send home a lot of paper packets that contained prewriting and drawing practice worksheets. I have since stopped. Why? So much learning comes from experiences that do not involve pencil and paper and summer is the perfect time to explore that! Kids NEED to experience more hands-on activities and play in order to have strong muscles for pencil and paper tasks. Instead of completing writing worksheets, try suggesting students use sidewalk chalk or draw shapes and letters in the sand. You can also recommend families try some of these easy gross and fine motor activities using household items!
3. Focus on Life Skills
Summer is the perfect time to work on various household tasks and life skills, such as cooking, cleaning, and even community outings. For sensory sensitive kids, some of these tasks can be very overwhelming. One of the pros of a slower summer schedule is there may be more time and flexibility to gradually build confidence and skills to be able to engage in some of these tasks.
4. Make it Routine
Routines and themes help me stay on track during the school year, and I like to suggest the same to my families for the summer. Depending on your student, you may recommend a few activities for families to focus on consistently in daily or weekly routines. Some years, I have recommended daily ‘themes’ and corresponding activity ideas such as Movement Monday, Fine Motor Tuesday, Sensory Wednesday, Cooking Thursday, Community Outing Friday. Families can choose one activity per day based on the daily theme. Or, you could collaborate with a family to choose 1 or 2 daily routines to target and recommend a therapeutic spin on it. For example, when reading books at bedtime, have the student lay on his tummy. During the morning routine, try to encourage decreased verbal prompts. This way, activities don’t feel like ‘extra’ work because they are already embedded into activities that happen in the family on a daily basis!
5. Keep it Simple
This is probably the most important tip of all. Let’s face it. It has been a long school year! While some families may be looking for very detailed activity plans, others may be looking for a few practical ideas. In general, I like to recommend simple, actionable ideas that can be easily implemented and don’t require a lot of preparation and planning. Like everything, touch base with your families and see where they may be looking for support and you can tweak your plan from there. I recommend starting simple and adjusting as needed to meet individual needs.
About the Author:
Katie McKenna, MS, OTR/L is an occupational therapist working with students in the school setting. Katie has worked with students of all ages, from early childhood up to high school transition. Before she was an OT, Katie worked as an in-home respite worker as well as an inclusion aide. Katie earned an undergraduate degree in Communication Sciences and Disorders from Saint Louis University, and a Masters degree in Occupational Therapy from the University of Illinois at Chicago.
By: Rosemarie Griffin, SLP, BCBA, originally posted on ABASpeech.org
Play is this fascinating tool that allows children to absorb information, learn, engage, socialize, and communicate. Play is vital to children’s development. Play is a natural way to bring children into an exciting new adventure each day. When discussing play skills development, caregivers and providers often need a refresher on what play skills are appropriate for various ages. Play can give children a sense of closeness when playing, build social skills, problem solving skills, and of course learn language. Understanding the stages of play skills development can help with knowing what play is appropriate and when!
Milestones of Play
6-12 months- In this baby stage, play is simple, but so rewarding for the child and parent! Imitation is a huge deal at this age and children love to imitate anyone they are playing with. Think of games like “so big” or simply waving. Playing peek-a-boo is so much fun and a great way to engage in play with little ones. Songs with silly words are wonderful at this age also. Remember communication and play starts well before language, so nonverbal play is hugely important too!
18 months- Here comes the pretend play! Toy kitchens are all the rage for our blooming toddlers because pretend play is blossoming and imaginations are growing. Our toddlers begin to use tools like hammers or spoons to imitate real life actions in their pretend play. Feeding our baby dolls is another big one at this stage! Often this age group engages in solitary play and will build blocks alone or complete a puzzle by themselves. They often don’t even notice if other children are around them!
2 year olds- Now that our children are a bit bigger, they are ready to engage in even more developed pretend play. Now children may imitate household chores like pretending to sweep or wash the dishes. This would be the perfect time to play house and use their world in their pretend world!
Onlooker Play- When children are preschool age, they may begin to watch other children play and this is called onlooker play. Onlooker play is when children watch other children play! During this time, children are building their social and emotional skills and also learning how to engage in situations. They are even learning from other children and boosting attention and memory!
Parallel Play-This is another play development around ages 2-3 when children are playing next to each other, maybe with the same toys, but not engaging with one another. The children influence each other and may even copy each other! Think of this as a precursor to learning how to truly play together!
Associative Play- Between 3-4 children begin to play together by using the same materials and doing similar activities, but they are still a bit independent. Think two children sharing crayons, but drawing sepapare pictures. The children like the company of the others, but aren’t ready to actually make a game together yet.
Cooperative Play- Lastly, between 4-5 children start to interact with one another and play together! They want the interaction and they want to do the activity together. This is where pretend play really takes off and children pretend to be the mom and dad and take care of a baby or serve each other dinner at the pretend restaurant!
Play and Therapy
The most important idea to remember when it comes to play in therapy is that it is all about the mindset. Don’t be afraid to get silly. Loosen up! Make silly faces, use silly sounds, and make those genuine connections. Toys aren’t as important as human connections, so don’t worry about all the toys and just be you! If you are looking for a few toys though, bubbles, balls and markers are great ideas! Puppets can be a ton of fun too! Stay away from anything that needs batteries because that takes the play away from the child. The toy does all the work! The more content that is introduced while playing, the more the child will remember and absorb from you!
When it comes to play skills development, it is so important to understand the age of the child and the impact play will have on them. It is also so important to know what to expect in terms of play from a child at different age groups. Play is such a huge stepping stone in learning, engagement, social skills, and communication. Play skills development is a great topic to delve into if you are a parent or a SLP!
Rosemarie Griffin, SLP, BCBA is dedicated to helping SLPs and other professionals provide systematic language instruction with ease. Working with students with autism and other complex communication disorders can be challenging. Rose has dedicated herself to helping by providing professional development and real life examples of what she does in her daily practice. See her podcast, blog, and collaboration opportunities at www.abaspeech.org
As adults, we’re fairly accustomed to contracts for car loans, new employment, or updates to our smartphones. But contracts can also be beneficial in the classroom setting. A contingency contract is defined as “a mutually agreed-upon document between parties (e.g., parent and child) that specifies a contingent relationship between the completion of specified behavior(s) and access to specified reinforcer(s)” (Cooper, Heron, & Heward, 2007). There are several studies that indicate using a contingency classroom can be beneficial in the classroom setting.
This allows you to work together to identify problem behaviors to be addressed, identify the contingencies currently maintaining these behaviors, determine the child’s current reinforcers, and establish what reinforcement or punishment procedures will be used.
Use this information to create a clear, complete, and simple contract.
The authors provide examples of how these contracts might look. You can vary the contract based upon the behaviors you are addressing with your student and the student’s ability to comprehend such contracts.
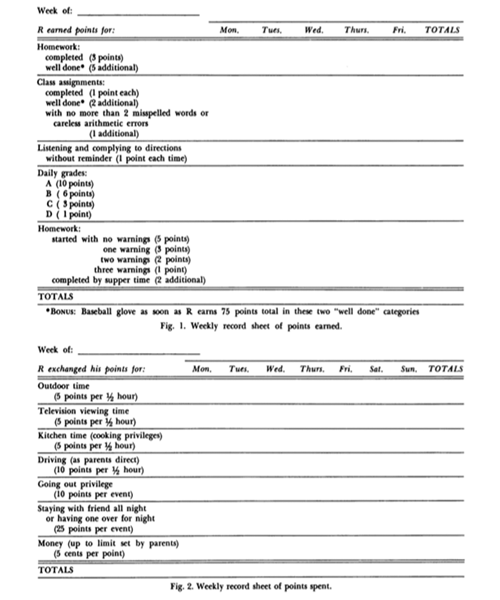
Build data collection into the contract itself.
You can see an example from the article below. For this example, it is clear how points are earned and how the child can utilize those points, and the contract itself is a record of both the points and the child’s behaviors.
There are clear benefits to utilizing such contingency contracting: building relationships across different environments in which the student lives and works, addressing one or more challenging behaviors simultaneously, and providing opportunities for students to come into contact with reinforcement. You can read the entire article here:
Cantrell, R. P., Cantrell, M. L., Huddleston, C. M., & Wooldridge, R. L. (1969). Contingency contracting with school problems. Journal of Applied Behavior Analysis, 2(3), 215-220.
And much more has been written about contingency contracting. If you’d like to learn more, we suggest taking a look at one or more of the following:
Bailey, J. S., Wolf, M. M., & Phillips, E. L. (1970). Home-based reinforcement and the modification of pre-delinquent’s classroom behavior. Journal of Applied Behavior Analysis, 3(3), 223-233.
Barth, R. (1979). Home-based reinforcement of school behavior: A review and analysis. Review of Educational Research, 49(3), 436-458.
Broughton, S. F., Barton, E. S., & Owen, P. R. (1981). Home based contingency systems for school problems. School Psychology Review, 10(1), 26-36.
Miller, D. L., & Kelley, M. L. (1991). Interventions for improving homework performance: A critical review. School Psychology Quarterly, 6(3), 174.
About the Author:
Sam Blanco, PhD, LBA, BCBA is an ABA provider for students ages 3-15 in NYC. Working in education for twelve years with students with Autism Spectrum Disorders and other developmental delays, Sam utilizes strategies for achieving a multitude of academic, behavior, and social goals. She is also an assistant professor in the ABA program at The Sage Colleges. You can read more of Sam’s posts for Different Roads To Learning by clicking here!