This month’s ASAT feature comes to us from Shira Karpel, MEd, BCBA and Shayna Gaunt, MA, BCBA, How to ABA. To learn more about ASAT, please visit their website at www.asatonline.org. You can also sign up for ASAT’s free newsletter, Science in Autism Treatment, and like them on Facebook!
I’m a newly certified behavior analyst working in a school-age program. Many of my students struggle with emotion regulation. However, my coursework and supervision were primarily focused on easily measurable, observable behaviors. While I was taught that behavior analysis doesn’t discredit private events, I just don’t know where to start. A few initial topics or tools for teaching emotion regulation would be helpful to get me started.
A Brief Review of Emotion Regulation
We cannot ignore that children have emotions. As behavior analysts, we are trained to study behavior that is observable and measurable – not private events like thoughts and emotions. But how can we ignore that some of the students we work with are struggling with managing how they are feeling? We need to allow our students to have these emotions, but it is also important to teach them coping strategies and emotion regulation techniques. In terms of social significance, this is a big one!
Individuals with ASD have more emotion regulation difficulties and consistently demonstrate less adaptive regulation strategies, as well as internalizing problems such as anxiety and externalizing problems such aggression (Cai et al., 2018). Emotion regulation is the ability to do hard things despite some uncomfortable feelings. It’s the ability to use strategies in dealing with emotions like disappointment, frustration, and anger – and being able to recover. It’s a form of resilience that many of our learners would benefit from learning.
Yes! As behavior analysts, we only implement strategies and programs to address emotion regulation that are evidence-based.
Yes! We need to be able to describe these behaviors in ways that are observable and measurable.
Yes! We need to continuously take data and analyze the data to make any necessary changes.
According to Skinner (Verbal Behavior, 1957), private events are considered behaviors that are under the control of environmental stimuli and can be defined in behavioral terms. Skinner noted that radical behaviorism “does not insist upon truth by agreement and can therefore consider events taking place in the private world within the skin. It does not call these events unobservable” (Skinner, 1974, p. 16).
In line with Skinner’s definition, emotions, and emotion regulation are private events. They are under the control of environmental stimuli, but they can be defined and measured. Let’s take ‘anxious’ for instance. ‘Anxious’ should be individually defined for each person, including observable and measurable events like flushed cheeks, red ears, and ringing of one’s hands in a particular way. Likewise, emotion regulation could be defined as using strategies like counting backward or taking three deep breaths.
So, how can we talk about feelings and teach emotion regulation strategies in a behavior-analytic way? Before we review 7 of our favorite strategies, it is very important to collect some baseline data on common triggers and setting events as these situations will inform your practice sessions and your efforts to promote generalization of the regulation skills being targeted.
7 Strategies for Emotion Regulation
The strategies for emotion regulation are best taught when a student is calm, and supported and modeled while their emotion experience is occurring. Then, it can be generalized to times when the student is more dysregulated. We don’t know about you, but when we are very upset, it only makes us feel worse when someone tells us to “calm down” or “relax.” During the heat of the moment, we’re not thinking straight. Find a moment when the student is calm and make learning into a positive experience. Here are some teaching techniques:
- Identify and Teach Prerequisite Skills: Teaching emotion regulation in ABA requires foundational skills such as basic communication (i.e., the ability to get one’s needs met), understanding reinforcement (i.e., the first/then contingency), impulse control, self-awareness, and the ability to recognize emotions in oneself (Conallen & Reed, 2016). Building these prerequisite skills is necessary to ensure that learners can understand more complex concepts when you begin to teach emotion regulation strategies.
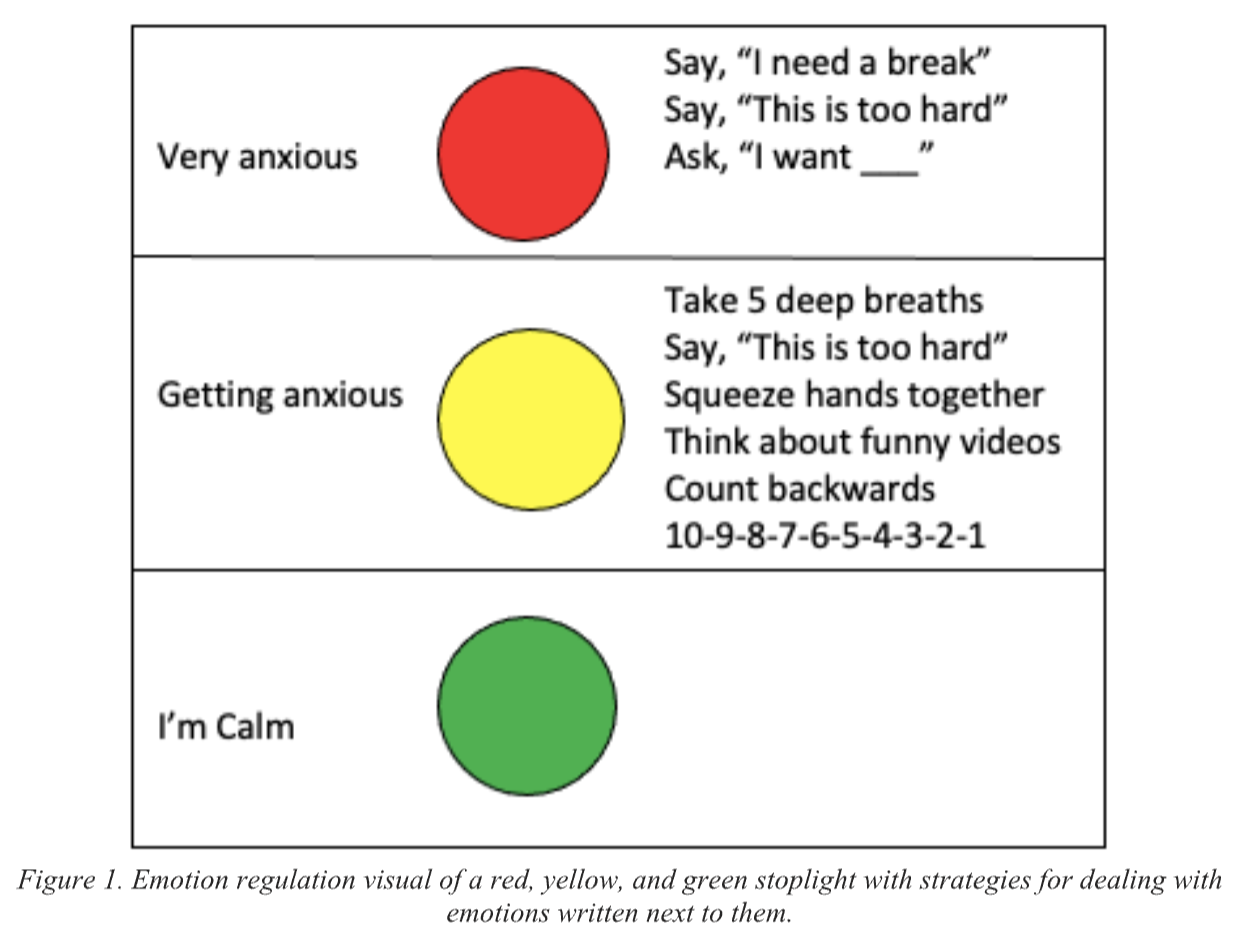
- Teach Using Visuals: Visual supports, like photographs, icons, text, and video, are an evidenced-based strategy used to teach children with ASD new skills by providing cues (Hume et al., 2014). We can’t assume that a child knows what “anxious” or “frustrated” means. When teaching abstract concepts such as feelings, it is important to use visuals. Using visuals while teaching enhances understanding, supports communication, facilitates memory and recall, and increases engagement, making learning more effective and less anxiety-inducing (Beaumont & Sofronoff, 2008).There are different ways to do this depending on the age and skill of the learner. For example, you can show videos of people who are angry, anxious, and frustrated and label those videos. You can have students identify and match emotions to various situations (Conallen & Reed, 2016). Hint – for maximum success, start with emotion words that the student has already learned. Then, build in other target words that may be more accurate or nuanced from there.The stop light visual depicted in Figure 1 is an example of something that you can use to support teaching. Red, yellow, and green correspond to different emotional states. If the student can read, calming strategies can be written right beside the colors. Be sure to pair this visual with evidenced-based teaching such as prompting, modeling, and differential reinforcement.
For younger students, we have used a simple flip book with small circles corresponding to different emotional states. On the front of the circles is a picture of the emotion and on the back are pictures of different calming strategies. With prompting and fading, the student can learn to flip to the color that they are feeling and then engage in calming activities. (See Figure 2 for a visual example.) - Model Labeling Behaviors: Modelling has long been used as an effective prompt in applied behavior analysis (Brody et al., 1978). Model labeling your behavior and your student’s behavior. When something happens to frustrate you, say something like, “I’m feeling so frustrated, I need to take some deep breaths to calm down.” If a student sits calmly, say, “I like how calmly you’re sitting. You look like you’re feeling green and calm,” while also pointing to the green circle. Or, if they are upset, say, “Your shoulders are raised, it seems like you’re heading towards yellow and feeling upset,” and casually flip their circle to yellow. At this point, there is no demand on the student other than to tolerate you making the comments.
- Discrete Trial Teaching: In addition to labeling emotions in situ (in natural settings versus “tabletop”) using visual supports, formal teaching may need to happen. Using discrete trial teaching, teach the student to receptively identify the different colors and corresponding feelings. For example, for receptive identification, you can put out all 3 circles and say, “Show me the angry circle.” For expressive identification, you ask the student to label the emotion depicted in your materials. For example, follow up by asking, “What is this circle?”. You’ll also be asking them to label how they are feeling. “You look like you are yellow. How are you feeling?” For more on the efficacy of discrete trial teaching and some current guidelines, refer to Leaf et al. (2017). Use evidenced-based practices such as prompting, prompt fading, and differential reinforcement to teach this. With proper shaping and prompt fading, the student should eventually be able to identify and label their behavior receptively, and then expressively. To learn more about teaching receptive skills, please check out the blog on receptive labels.

- Behavior Skills Training (BST): When the student is calm, use behavior skills training (Sarokoff & Sturmey, 2004) to teach positive replacement behaviors that will help regulate their emotions. BST involves four components: Instruction, Modeling, Rehearsal, and Feedback.
a) Instruction: Give a brief explanation of why these calming strategies are important. If a student doesn’t understand the language, skip the wordy explanation.
b) Model: Then model some calming strategies.
c) Rehearsal: Practice by role playing behaviors together, such as “taking deep breaths,” “counting to 5,” “going for a walk.” etc. These may need to be individualized to the learner as you figure out what calms the student. Incorporate choice. Which techniques does your student like best?
d) Feedback: Give the student lots of positive feedback, and only one piece of corrective feedback to work on. Do this a lot in practice sessions and slowly start helping the student use these strategies when they are beginning to get heightened. Initially, this task will be teacher-directed (i.e., the instructor may have to prompt the student to respond). However, the ultimate goal is to have the student demonstrate this response independently. - Give Feedback: Give the student feedback on how they’re doing. Reinforce behaviors such as “using calming strategies” or “letting others know how you feel.” It is important that praise is not given for being calm. The message should be that it is okay to feel those other emotions, it is just not okay to engage in challenging behavior when you have those feelings. If there is an episode of negative behavior where the regulation strategies were not used, debrief on that too. When the student is calm, review the incident and talk about how they can make it better next time. Use visuals for these conversations. And remember – they don’t need to be fancy. Draw it out in the moment, using stick figures and chicken scratch printing. You can visually depict the result of using the strategies and calming down versus not using the strategies. Then, you can role-play the scenario to practice how they can make it better next time.
- Promote Generalization of the Skills to the Environment: Set up practice situations in novel environments and with novel people so that the student can practice using the strategies and accessing reinforcement for the behaviors they are displaying. Make sure you have visuals while you’re practicing. Look back at the common triggers that you noted during your baseline assessment. Are these new skills being used in those situations? If not, layer in practice using the above strategies so that generalization is more likely to be observed.
Measuring Progress
Data collection is also an important component of teaching emotion regulation. You should take data on things like:
- Frequency of challenging behavior (it should decrease as the learner gets more proficient with self-regulation)
- Duration of peak challenging behaviors from onset until offset (or until calming strategies are used)
- Antecedent triggers to challenging behavior (knowing this information can guide how you teach generalization of regulation skills)
- Level of independence with identifying their emotional state (i.e., how much prompting was needed, if any)
- Level of independence by engaging in a calming down routine
- Ability to generalize to novel environments and people
In Summary
When teaching emotions and emotion regulation, we want to first define these private events using observable and measurable terms. Then, it’s important to use evidenced-based teaching practices such as the use of visual supports, modeling, prompting, prompt fading, differential reinforcement, and behavioral skills training. Once our students have a better understanding of emotions, we want to teach our students that it’s okay to have these feelings. We want to help them understand them, express them, and then manage them. The goal is that they will use replacement behaviors such as calming techniques when they are feeling anxious, angry, etc. instead of engaging in challenging behavior. With successful teaching and practice, students can become masters of their own behavior! As a new behavior analyst, we wish you all the best!
References cited above:
Beaumont, R., & Sofronoff, K. (2008). A multi-component social skills intervention for children with Asperger syndrome: The Junior Detective Training Program. Journal of Child Psychology and Psychiatry, 49(7), 743-753. https://doi.org/10.1111/j.1469-7610.2008.01920.x
Brody, G. H., Lahey, B. B., & Combs, M. L. (1978). Effects of intermittent modelling on observational learning. Journal of Applied Behavior Analysis, 11(1), 87-90. https://doi.org/10.1901/jaba.1978.11-87
Cai, R. Y., Richdale, A. L., Uljarević, M., Dissanayake, C., & Samson, A. C. (2018). Emotion regulation in autism spectrum disorder: Where we are and where we need to go. Autism Research, 11(7), 962-978. https://doi.org/10.1002/aur.1968
Conallen, K., & Reed, P. (2016). A teaching procedure to help children with autistic spectrum disorder to label emotions. Research in Autism Spectrum Disorders, 23, 63-72.https://doi.org/10.1016/j.rasd.2015.11.006.
Hume, K., Wong, C., Plavnick, J., Schultz, T. (2014). Use of Visual Supports with Young Children with Autism Spectrum Disorders. In: J. Tarbox, D. Dixon, P. Sturmey, & J.Matson, J. (Eds). Handbook of Early Intervention for Autism Spectrum Disorders. Autism and Child Psychopathology Series. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-0401-3_15
Leaf, J. B., Cihon, J. H., Leaf, R., McEachin, J., & Taubman, M. (2017). A progressive approach to discrete trial teaching: Some current guidelines. International Electronic Journal of Elementary Education, 9(2), 361-372. Retrieved from https://www.iejee.com/index.php/IEJEE/article/view/163
Sarokoff, R. A., & Sturmey, P. (2004). The effects of behavioral skills training on staff implementation of discrete trial teaching. Journal of Applied Behavior Analysis, 37, 535-538. https://doi.org/10.1901/jaba.2004.37-535
Skinner, B. F. (1957). Verbal behavior. Appleton-Century-Crofts.
About the Authors:
Shira Karpel, MEd, R.B.A (Ont), BCBA is the co-founder and director of How to ABA, an online resource and community for ABA professionals. Shira has a Masters in Special Education and has been in the field of ABA since 2011, receiving her BCBA in 2014. Together with Shayna, they trained and taught many therapists, clients, and parents and collected a massive bank of ABA programs and resources. In an effort to give back to the field, Shira and Shayna decided to create How to ABA as a way of sharing our collection of resources with others. As a former teacher, her passion is in using ABA in classrooms in order to create positive and comprehensive learning environments for all students. She is the Clinical Director at a private school in Toronto and is loving getting to make a difference in the lives of children and families daily. She is passionate about making the principles of ABA practical, doable and relevant to every child in any situation.
Shayna Gaunt, MA, R.B.A (Ont), BCBA is a dedicated professional in the field of Applied Behavior Analysis (ABA) and co-founder of How to ABA, an online resource and community supporting ABA professionals. With over two decades in the field, a Master’s Degree in ABA from the University of Nevada Reno, and extensive international experience, Shayna brings a vast expertise across diverse settings. She emphasizes collaborative excellence in direct therapy, supervision, and training, striving to deliver high-quality services and resources to clients and fellow ABA practitioners. Through How to ABA, Shayna aims to make ABA principles accessible and practical, fostering a community where professionals can share, learn, and grow together.