Category Archives: Autism Awareness
Double Up!
Learn all about our newest game Double Up from creator Rosemarie Griffin, CCC/SLP, BCBA!
If you are working with older students, I know that you have probably struggled with finding materials that were age appropriate. I am a school based speech language pathologist and board certified analyst. I created Double Up to help my students strengthen their vocabulary and leisure skills.
If you are a special education teacher, speech language pathologist, board certified behavior analyst or parent – you will love Double Up. This product can be used with students who are non-verbal and by students who are conversational. A no prep social skills activity for mixed groups!!
Double Up includes 4 different games and 144 vocabulary cards. It can be played with as few as one person or as many as 4 people. Vocabulary terms focus on the areas of leisure and hygiene. The first person to fill up their board- yells “Double Up” and they are the winner. Read below for skills that you can work on when playing Double Up.

Matching – If you have students who would benefit from matching identical pictures, you can do that easily with double up! Just pass out the game boards of the same color. Get the matching vocabulary cards and you are ready to go. Each student picks a card and matches to their board. If they don’t have the card they pick – they can pass it to the person who does have it. If students are able to ask they can ask who has the card. For example, “who has the picture of reading?”

Associations – Students can work on matching items by association. If you pass out the purple leisure noun boards, get out the red leisure action vocabulary cards. You will turn over a leisure action ( i.e. reading), if you have the picture of the book on your board – you match it! If someone else has the book – you can pass it to them or ask “who has the book?” A great way to play for students who understand word associations.

Turn Taking – Double Up allows for practice with turn taking. Picking a card and taking your card is a functional leisure skill. The format of this game, allows for many opportunities to take your turn and wait while others take their turn.
Waiting – If you play Double Up as a 4 person game- your students will have to wait for their peers to take a turn. This is a natural way to work on the skill of waiting. Waiting can be so very difficult for our students and this is a great way to embed work on this skill.
Independent Work. Double Up also makes a functional independent work task. A student could take one board from the double up game and the matching cards. They would match the identical cards for an independent work task. The pictures are functional and age appropriate, so not only are students work on increasing their duration with an independent task, they are being exposed to words that are important to them!
Conversation Skills – The pictures in double up lend themselves to conversation. You can discuss the vocabulary terms with the students. “Have you lifted weights before?” “Have you been camping?” The conversation opportunities are endless!
About the Author
Rosemarie Griffin, MA, CCC/SLP BCBA, is an ASHA certified Speech-Language Pathologist and a Board Certified Behavior Analyst. She divides her time between a public school and a private school for students with autism in Ohio. She’s presented at the national, state and local level about systematic and collaborative language instruction for students with autism. Her professional mission is to help all students expand their communication step by step. She can be reached at www.abaspeech.org, on Facebook or Instagram.
3 Ways To Fade Prompts
Prompts are ways we help our learners demonstrate new skills. We use prompts to get our students to greet a peer, flush the toilet, name the color blue, and clap their hands. Prompts are something we add to the situation because the natural or teaching cue was not enough to cause the student to respond. The natural cue of being finished using the toilet was not a strong enough reminder to flush the toilet so we added the verbal prompt, “flush the toilet” and the student now responds. Prompts are important but fading them is just as important. Prompt fading in ABA needs to be planned from the start and is an integral and essential component to the plan. Unless you are committing to following that child around for the rest of his life and tell him to flush the toilet – prompt fading is essential.
Some rules for prompt fading in ABA:
* Plan it out from the start.
* Train your staff.
* Do it gradually.
* If incorrect responding begins, return to last prompt level.
1. Least to Most Prompt Fading
Like we discussed in Monday’s post, least to most prompting involves starting with the least intrusive prompts and moving up in the prompting hierarchy. This can be beneficial because it gives students to the opportunity to be independent and you are only providing as much prompting as needed. This is a strategy we tend to use naturally. When you meet a your friend’s toddler you put out your hand to give a high five. If she doesn’t respond you say, “give high five.” If she still doesn’t respond you move her hand to your hand to give a high five. This is a natural method of prompting. When using this prompt fading technique, ideally the prompts will be somewhat self fading. If you are always starting at the least intrusive prompt, your students will have the opportunity to demonstrate independence. As the student begins to learn the task, he will need less and less prompts to perform it correctly.
Some key tips for using this prompt fading in ABA procedure:
- allow wait time; if you do not provide wait time you may be providing more prompts than needed and taking away the opportunity for the student to respond correctly
- take data; data is key to track progress. Every time you utilize this prompting method – note the level of prompt you used. You want to see that your student is requiring less intrusive prompts as time goes on. This will help avoid prompt dependence.
- use high powered reinforcers; use an item that is actually a reinforcer that your student wants to work for. The sooner he demonstrates the skills, the sooner he gets the reinforcer.
2. Most to Least Prompt Fading
Most to Least prompt fading is another effective method of using prompts. With this method you start the most intrusive prompts and gradually fade to less intrusive prompts. The prompt fading is build right in. However, sometimes people forget that and in their head rename this most to most prompting. The key to errorless learning and using the most intrusive prompts first is that you fade the prompts out. The idea behind most to least prompting is that students will contact reinforcement right away and you will avoid errors and the students developing any incorrect habits.
How to fade prompts in Most to Least Prompting:
- set criteria for changing prompts; once your student hits a particular number of days or sessions or trials at a particular prompt level, fade to the next level; take data to track progress
- once you hit the criteria move to the next type of prompt; refer to our prompt hierarchy or order that is in Monday’s post. Move up the list to less and less intrusive prompts.
- fade magnitude than switch prompt type; before you switch from a gestural to a verbal prompt adjust the magnitude of the prompt. A dramatic point to an object is different that a nod of your head.
Data is critically important for avoiding prompt dependence. You want to set a criteria ahead of time and take data to make sure you are sticking with the criteria. The criteria you set will depend on the student and the task. Maybe you want 3 consecutive days with each prompt level. If you are taking data you can ensure that you are sticking to that schedule. If errors begin occurring, go back a prompt level. The data will guide your implementation of this procedure. If you are fading too quickly, your data will tell you!
Prompt fading in ABA isn’t scary. Plan ahead and make sure you train your staff. This is a group endeavor!
3. Time Delay
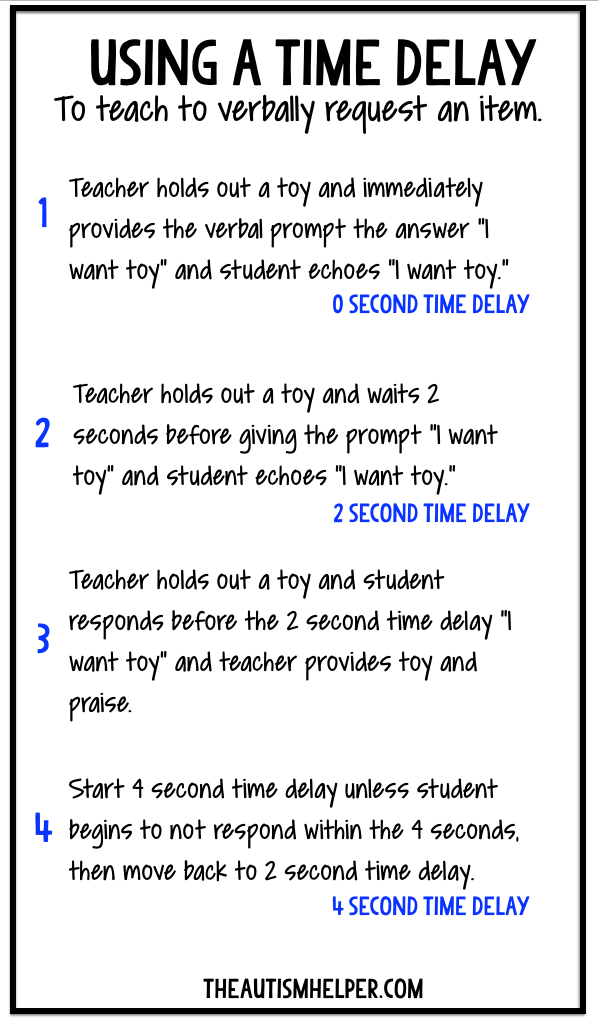
One effective way we can fade prompts is using a time delay. A time delay inserts a set amount of time between the natural or teaching cue and our prompt. When utilizing a time delay, start with a zero second (i.e. no) time delay – so it will basically be like errorless teaching. For the first few trials, give the prompt right away so the student knows how to respond. Then after several trials, increase the time delay. For example, you may start with 2 seconds. If the student does not respond within 2 seconds – provide the prompt. If the student responds before the 2 seconds, provide loads of reinforcement. Once the student is successful and responding under the 2 seconds for several trials, increase the time delay. Now wait until 4 seconds to provide the prompt. Continue on. If the student does not respond with the 4 second time delay, move back to the 2 second time delay.
The key to time delay is planning and data. Set the criterion ahead of time. Plan how many sessions you will do at 0 seconds before moving to the first time delay. Determine what the mastery criteria is – how many times do you want the student to respond within the time delay before increasing the time delay length? Take data on this. It can easily and quickly get confusing if you don’t have a data sheet to track what you are doing. Write the plan in simple terms at the top of your data sheet. I like to track prompted correct (PC), prompted incorrect (PI), unprompted correct (UC), and unprompted incorrect (UI) using those abbreviations on my data sheet. If the student responds before the prompt it is counted as unprompted and if it’s after the prompt it is prompted!
There is no magic number of trials or days you should stay within the 0 second or 2 second time delay. It depends on the student’s level of functioning and the difficulty of the task. This is where data majorly comes in to play. If you’ve moved along too quickly, you will know and you can scale back.
Time delay works really well with verbal prompts. Another key component to time delay working successfully is making sure the reinforcement you give for the unprompted responses is better than the reinforcement for prompted responses. So if Johnny responds before the time delay and says the color blue on his own – give him 3 m&ms and praise but if you are using a 2 second time delay and he doesn’t respond and you provide the verbal prompt “bl…” and then he says blue only provide praise. You want the independent responses to be getting more reinforcement so your student is motivated to engage in those responses more!
About The Author
Sasha Long, BCBA, M.A., is the founder and president of The Autism Helper, Inc. She is a board certified behavior analyst and certified special education teacher. After ten years of teaching in a self-contained special education classroom, Sasha now works full time as a consultant, writer, and behavior analyst. Sasha manages and writes The Autism Helper Blog, as a way to share easy to use and ready to implement strategies and ideas. Sasha also travels internationally as a speaker and consultant providing individualized training and feedback to parents, educators, therapists and administrators in the world of autism. She is currently an adjunct professor in the school of Applied Behavior Analysis at The Chicago School of Professional Psychology. Sasha received her undergraduate degree in Special Education from Miami University and has a Masters Degree in Applied Behavior Analysis from The Chicago School of Professional Psychology. Contact Sasha at sasha.theautismhelper@gmail.com.
Super Sensory Sale!

Save 30% on select fidgets, weighted toys, and other sensory supports! Now through October 29th!
Normalization
So much to say on this topic, far more than anyone would actually want to read.
Does ABA therapy require/demand/force individuals into a narrow and specific box titled “NORMAL”? No.
(Well, it shouldn’t anyway)
But the myth persists.
I mean this in the best way, but many of the children I work with just are not going to fit into that “normal” box, no matter how much someone tries to push or squeeze them into it… it ain’t happening.
And that’s a cause for celebration!
The very thing I love about working with such a diverse group of kids, is that they are all different, yet all interesting. I work with some super fascinating small people, who constantly show me how dumb I am. And I thank them for it, because how can you grow if you already think you know everything? You can’t.
As a provider, of course I know the research on the effectiveness of ABA therapy. I also know the many success stories I have seen with my own eyes, of children I directly worked with. But success story does not equal “…and then the child was totally normal!”.
A couple of reasons why my job is not to drive families in my car to a fantasy location called “normal”:
1) Each client/family I work with usually has their own idea of what “normal” means. If you have been in this field more than 10 minutes, you know this to be true. This client over here may live in a home where no one really cares what time they go to bed, as long as they stay in their room and are quiet. But that client over there, may live in a home where all the parents want most in the world is for that child to get their 7.5 hours of sleep every night.
2) Even when a family can explain to me what “normal” means for them, it quickly changes! Again, if you have been in this field more than 10 minutes you know this is true. Sometimes parents tell me they want desperately for their child to talk, but what they really mean is they want their child to communicate. Or, a parent may tell me they want desperately for their child to go to “normal” school with their big sister, but next thing you know that parent has decided to homeschool. Expectations change, as perspective changes.
So if ABA therapy is not about hitting a child over the head with your magical “normal” baseball bat, then how exactly is it decided what the goals of treatment will be? I’m so glad you asked.
If you are working with a quality ABA provider, the goal selection process will look something like this:
“I need to evaluate/assess your child to collect baseline data” – This just means data is collected at the onset of services to create a starting point. Over time, that starting point data will be reviewed again and again to make sure the child is progressing. If therapy has been happening week after week after week, but the child has not progressed past that starting point, then something is seriously wrong. This is why it’s important to collect that initial data, so over time you can compare the child’s current learning to their previous learning.”
“What are your goals for therapy? Tell me the reasons why you initiated services.” – The people who asked the ABA team to show up clearly had reasons for doing so, and we need to know what those reasons are. We cannot fully help if we don’t know what issues are happening. Treatment planning should always be a team effort, with the family/client working together with the BCBA to create goals.”
“What are the highest priority areas of concern in the home? At school? In the community?” – What this question is really getting at is “where do you want to start?”. It isn’t unusual that families want to work on…oh, 85 behaviors or so when you first meet them. Unless I can get a good idea of the priority level of those 85 things, the treatment plan will be a chaotic mess. Prioritizing treatment helps focus in on the areas of deficit that are impacting the client the most.
“Describe your household: rules, routine, disciplinary procedures commonly used, etc.” – This question gets at Culture. Households form a sort of culture, or a way things are done. Stepping into a household/family dynamic and imposing completely opposing culture onto it, is not a great idea. It will likely lead to aggressive resistance. What is more helpful, is to teach the family strategies and techniques that line up with the way their household functions.
“Can you finish this sentence: In 5 years, I want my child to be able to…..” – This question is really getting at long-term goals. Professionals need to know long-term goals, because every long-term goal is really made up of hundreds of baby steps. Gradually introducing those baby steps leaves less work to do down the road and increases the likelihood of successful skill acquisition.
“Your child scored low on (insert skill domain here). Do you care about that??” – One of my fave questions to ask. I have learned to ask this, because I used to do quite a bit of assuming. Things like “Of course, you guys want him to write his name, right?” or “Of course, you guys want her to stop eating with her hands, right?”. Maybe not. If I see an area of concern, I will bring it up. If the parent isn’t as concerned as I am or wants to stick a pin in that issue until a later time, then it’s really important that I know that.
My normal is not your normal, and vice versa. What’s considered “normal” in your household might not fly in my household, and what’s “normal” in your marriage could be unbearable for another couple. That’s why normal is such a useless word to throw around, because it has too many meanings to actually mean anything significant.
One of my pet peeves is when a parent says to me during an intake, “I just want him/her to be normal!”. Ummm, and that means what?? 🙂 Seriously, I need details over here. I do not have an intervention for “normal” behavior, nor do I know how to program for that.
Does ABA therapy seek to change individuals? Yes! Behavior change is the entire point of this therapy, either increasing appropriate behaviors or decreasing inappropriate behaviors. But if you think that the only change ABA therapy values is when a child can be fully “normal”, you are:
100%,
absolutely,
wrong.
About The Author: Tameika Meadows, BCBA
“I’ve been providing ABA therapy services to young children with Autism since early 2003. My career in ABA began when I stumbled upon a flyer on my college campus for what I assumed was a babysitting job. The job turned out to be an entry level ABA therapy position working with an adorable little boy with Autism. This would prove to be the unplanned beginning of a passionate career for me.
From those early days in the field, I am now an author, blogger, Consultant/Supervisor, and I regularly lead intensive training sessions for ABA staff and parents. If you are interested in my consultation services, or just have questions about the blog: contact me here.”
This piece originally appeared at www.iloveaba.com.
Pick of the Week: Games!

Implementing the Intervention…Even When Things are Going Well
Recently I was working with a parent who was using a TimeTimer with her son to help him recognize when it was time to get ready for bed. Our plan was to start the timer every night while he was engaged in an activity, show him the timer and have him repeat how many minutes left, then have him tell his mom when the timer went off. For the first couple of weeks, this plan worked beautifully. The boy could see the time elapsing, brought the timer to his mother when it went off, and then started the process to get ready for bed without engaging in tantrum behaviors.
I went in for a parent training session after a month of the intervention and the boy’s mother informed me the timer just wasn’t working any more. As we started talking, I realized that the mother had drifted from our original plan in a way that is quite common. As her son experienced success, she used the timer less frequently. Then, if he was struggling, she would introduce the timer. In effect, she started only using the timer when he was misbehaving, instead of using it as a consistent tool to help him with the bedtime routine.
This type of procedural drift (when there is an unintentional or unplanned change in the procedure outlined for the intervention) is very common for parents, teachers, and ABA therapists. It’s important to understand this type of drift so it can be corrected when it occurs.
Here are a few things to remember when implementing an intervention:
• First, any intervention should include a clear plan for fading the intervention. In the example above, the TimeTimer was an appropriate tool for this particular child, who was only four years old. But we don’t want him to rely on the timer for the duration of childhood! A plan should include how to fade the intervention with specific steps and specific requirements for mastery.
• The use of the TimeTimer is considered an antecedent intervention. This means that we are implementing a change in the environment prior to any problem behaviors to help the child contact reinforcement and experience success. Antecedent interventions should be implemented consistently as part of a routine, not ONLY when a problem behavior occurs. If it is only implemented when the problem behavior occurs, it is no longer an antecedent intervention.
• If we implement a tool (like the TimeTimer) only when problem behavior occurs, it’s possible the tool will become aversive to the child and possibly result in an increased magnitude of the problem behavior.
• Consider using tools for the people implementing to intervention to remind them of the specific steps. For example, you might create a video model and instruct the parent (or other adult implementing the intervention) to watch it every couple days. Or you might post the steps in a clear space to be reviewed regularly.
• Finally, we have to remember that a couple of good days in a row without any instances of problem behavior does not mean that the problem is solved. This is why the first step outlined above is so important. We want to teach the child replacement behaviors and give them lots of opportunities to be successful with it.
Ultimately, we were able to re-implement the procedure with this parent and see more continued success with this particular case. We also decided to post the steps to the intervention on the back of the TimeTimer for easy review on a daily basis.
However, in some cases, you might have to create an entirely new intervention using different tools. The goal is to be clear about the steps of the intervention, and to maintain those steps when implementing the intervention.
WRITTEN BY SAM BLANCO, PhD, LBA, BCBA
Sam is an ABA provider for students ages 3-15 in NYC. Working in education for twelve years with students with Autism Spectrum Disorders and other developmental delays, Sam utilizes strategies for achieving a multitude of academic, behavior, and social goals. She is also an assistant professor in the ABA program at The Sage Colleges.
How Parents Can Fit ABA Into Their Busy Schedules
“Dear Behavior BFF, I have followed your posts for a while now. The problem I see is that in order for me to be successful as a parent, I have to follow ABA 100% of the time. In order to be effective, do I need to enroll in graduate classes and learn everything I can about ABA? Do I need to become a BCBA to manage my own kids’ behavior better? Feeling overwhelmed over here…”
Thank you for learning about ABA as a parent. The science of behavior can help us SO much with our own kids. But does that mean you need to know every technical definition and fact before you can use some behavior strategies in your own home? NO! Heck no!
You are a busy parent. I am a busy parent. Most people reading this are busy parents (at least that’s the intended audience). Do you have time to complete a master’s degree in behavior analysis just to help you be a more efficient parent who capitalizes on the science of behavior? Ummm…no. You don’t have that kind of time. So does that mean you should give up on using behavior analysis as a parent? Also no.
Behavior analysis teaches us to focus on the behavior itself. It teaches us to manipulate the environment to help our kids engage in desired and proactive behaviors. It helps us find ways to increase positive reinforcement, increase positive interactions, and teach our kids to effectively communicate their wants and needs.
The good news is we can do all of those things within the constraints of our busy family schedules! You can use positive reinforcement effectively without knowing the difference between differential reinforcement of incompatible or alternative behaviors.
And more good news: when you need to get technical, there are Board Certified Behavior Analysts (BCBAs) to do that with you! We like talking behavior science. We are ABA nerds. Let us do that part for you. If you want to join us, then enroll in that ABA graduate program. If you don’t want a new career- then learn what you can as a parent in the time that you have.
So where do you start in order to not be overwhelmed and get the benefit of decades of behavioral research? You’re in the right place. Peruse these non-academic articles offered at bSci21 that help make the science easier to digest. Learn about positive reinforcement and how to use it effectively.
Start by providing positive reinforcement for desired behaviors. Decide what you want your child to do more of, then reward them for doing it! Start small with one behavior strategy at a time, then continue to learn and add another positive behavior support as you go.
You don’t have to become a behavior expert in order to effectively use behavior analysis to save your sanity as a parent. Start small, build a little at a time. Celebrate your successes. Reward your child(ren) for their successes. Shape your own behavior by building on with baby steps. Every step in the right direction is a success. Make it work for you and your family in the time that you have. You CAN do this!
About The Author
Leanne Page, MEd, BCBA, is the author of Parenting with Science: Behavior Analysis Saves Mom’s Sanity. As a Behavior Analyst and a mom of two little girls, she wanted to share behavior analysis with a population who could really use it- parents!
Leanne’s writing can be found in Parenting with Science and Parenting with ABA as well as a few other sites. She is a monthly contributor to bSci21.com , guest host for the Dr. Kim Live show, and has contributed to other websites as well.
Leanne has worked with children with disabilities for over 10 years. She earned both her Bachelor’s and Master’s degrees from Texas A&M University. She also completed ABA coursework through the University of North Texas before earning her BCBA certification in 2011. Leanne has worked as a special educator of both elementary and high school self-contained, inclusion, general education, and resource settings.
Leanne also has managed a center providing ABA services to children in 1:1 and small group settings. She has extensive experience in school and teacher training, therapist training, parent training, and providing direct services to children and families in a center-based or in-home therapy setting.
Leanne is now located in Dallas, Texas and is available for: distance BCBA and BCaBA supervision, parent training, speaking opportunities, and consultation. She can be reached via Facebook or at Lpagebcba@gmail.com.
Qualifications of Practitioners/Consultants who Practice ABA
This month’s ASAT feature comes to us from Sabrina Freeman, PhD, ASAT’s Consumer Corner Coordinator. To learn more about ASAT, please visit their website at www.asatonline.org. You can also sign up for ASAT’s free newsletter, Science in Autism Treatment, and like them on Facebook!
It’s crucial to be a savvy consumer when it comes to one of the most important decisions you will make for your loved one with autism – choosing an ABA treatment provider for your child. Those of us who have already walked in your shoes know that all treatment providers are not the same. To the uninitiated, these professionals all look marvelous. From the slick websites, to the large numbers of associations of which these professionals are members, it is becoming increasingly difficult to differentiate between mediocre and outstanding treatment providers. Furthermore, publication of research in high quality journals is not synonymous with clinical expertise.
Fortunately, in this issue of Consumer Corner, we present a summary of consumer guidelines created by the Autism Special Interest Group (SIG) of the Association of Behavior Analysis International to help you make an informed choice when searching for ABA professionals to design, run and maintain your child’s program. A complete copy of the SIG guidelines are available here: https://3lvvdfmmeol12qpvw2c75ch6-wpengine.netdna-ssl.com/wp-content/uploads/2018/07/Final-Autism-Sig-Guidelines-Parent-Version-May-2018.pdf It is important to remember that your child’s future depends on highly quality consulting. Good luck!
- Certification:
Treatment professionals must all have advanced degrees, e.g., a Master’s Degree or a Doctorate in a relevant field of study, and be certified either by the Behavior Analyst Certification Board (BACB), or a board that has equal or higher level requirements than the BACB. To look up your consultant, visit: www.bacb.com and click on “Find A Certificant.” If the potential consultant is not on this list, ask where he/she became credentialed, and trained so that you can verify licensure and experience to determine whether it is equal to/or surpasses the standards of the BACB. If this individual responds to your inquiry in a defensive manner, then you may consider looking elsewhere as you are well within your right to seek clarification about certification status.
- Extensive Hands-On Supervised Training:
Consultants are required to have extensive hands-on training treating children with autism in which they have worked at least one full year (1500 clock independent supervised hours or 1000 hours if taking a university practicum and 750 hours if taking an intensive practicum) under the supervision of a credentialed BCBA Certificant. In addition, they need to prove competency in many areas that cover the design and implementation of both individualized ABA interventions, and comprehensive ABA treatment programs. The partial list below was created by the Autism Special Interest Group (SIG) below. Your consultant should be competent in all the following areas:
- a) Design and implement individualized ABA Interventions
- community living skills
- functional communication skills (vocal and non-vocal)
- “learning to learn” skills (e.g., looking, listening, following instructions, imitating)
- motor skills
- personal safety skills
- play and leisure skills
- pre-academic and academic skills
- reduction of behaviors that jeopardize health and safety and impede successful functioning (e.g., stereotypic, obsessive, ritualistic, aggressive, self-injurious, disruptive, and other behaviors often described as “challenging”).
- school readiness skills
- self-care skills
- self- management skills
- social interaction skills
- vocational
- b) Design and implement both comprehensive ABA intervention programs (using multiple ABA procedures to address multiple intervention targets) and focused interventions (using one or more ABA procedures to address a small number of intervention targets).
- c) Delivering ABA interventions directly to at least 8 individuals with autism who present with a range of repertoires, levels of functioning, and ages.
- d) Implementing the full range of scientifically validated behavior analytic procedures, including but not limited to:
- reinforcement (including differential reinforcement)
- extinction
- discrete-trial procedures
- modeling (including video modeling)
- incidental teaching and other “naturalistic” methods
- activity-embedded intervention
- task analysis
- chaining
- activity schedules
- scripts and script fading
- prompting and prompt-fading
- errorless training
- error correction
- motivating operations
- stimulus control
- preference assessments
- choice
- augmentative and alternative communication training procedures.
- Continuing Education:
Not only do behavioral consultants need to be trained as above, in order to maintain their certification, practitioners must also pursue continuing education in a variety of areas that may include, but are not limited to, Applied Behavior Analysis.
Red Flag
These practitioners should not be working collaboratively with professionals who implement an eclectic mix of interventions that are untested, discredited or experimental in nature. If the consultant you use endorses an eclectic approach, understand that this practice is inconsistent with the BACB Guidelines for Responsible Conduct for Behavior Analysis. This red flag is a particularly helpful way to be forewarned about a consultant who is not a good choice to design and maintain your child’s program!
Common Mistakes In Implementing Reinforcement
Over the years, I’ve seen several behavior intervention plans written and implemented. Typically, these plans include reinforcement for the desirable behavior, but I see the same mistakes crop up again and again. Here are a few common mistakes in implementing reinforcement to look out for:
Fail to identify individual reinforcers. Hands down, the most common error I see is identifying specific activities or items as reinforcing. For instance, many people love gummy bears, but they make me want to puke. Presenting me with a gummy bear would not increase my future likelihood of engaging in the appropriate behavior! You must account for individual differences and conduct a preference assessment of your learner, then make a plan based on his or her preferences.
Fade reinforcement too quickly. Let’s say you’re working with a child named Harold who draws on the walls with crayon. You implement a reinforcement plan in which he earns praise and attention from his parent each time he draws on paper. The first few days it’s implemented, Harold’s rate of drawing on the wall greatly decreases. Everyone claims that his behavior is “fixed” and suddenly the plan for reinforcement is removed… and Harold begins drawing on the wall once more. I see this sort of pattern frequently (and have even caught myself doing it from time to time). After all, it can be easy to forget to reinforce positive behavior. To address this issue, make a clear plan for fading reinforcement, and use tools such as the MotivAider to help remind you to provide reinforcement for appropriate behavior.
Inconsistent with reinforcement plan. Harriet is writing consistently in a notebook, to the detriment of her interactions with peers. Her teachers implement a DRO, deciding to provide reinforcement for behavior other than the writing. However, the teachers didn’t notify all the adults working with her of the new plan, so Harriet’s behavior persists in certain environments, such as at recess, allowing her to miss multiple opportunities for more appropriate social interaction. To address this issue, make a clear outline of the environments in which the behavior is occurring and what adults are working in those environments. Ensure that all of the adults on that list are fully aware of the plan and kept abreast of any changes.
Don’t reinforce quickly enough. This one can be quite challenging, depending on the behavior and the environment. Let’s saying you’re working with a boy named Huck who curses often. You and your team devise a plan to reinforce appropriate language. You decide to offer him tokens that add up to free time at the end of the school day. However, sometimes as you are handing him a token for appropriate language, he curses again right before the token lands in his hand. Though it was unintentional, the cursing was actually reinforced here. Remember that reinforcement should be delivered as close to the desired behavior as possible. To address this issue, consider your environment and materials and make a plan to increase the speed of delivery.
Fail to make a plan to transfer to natural reinforcers. Ultimately, you don’t want any of these behaviors to change based solely on contrived reinforcement. Making a plan for reinforcement of appropriate behavior is essential, but your ultimate goal is to have the behavior be maintained by naturally occurring reinforcement. To address this issue, the first thing you need to do is identify what that naturally occurring reinforcement might be. For Harold, it might be having his artwork put up in a special place or sharing it with a show and tell. For Harriet it might be the interactions she has with peers on the playground. Once you have identified those reinforcers, you can create a plan for ensuring that the learner contacts those reinforcers over time. This might include pairing the naturally occurring reinforcers with the contrived reinforcers, then fading out the latter.
Ultimately, it’s important to remember that reinforcement is not as simple as it seems. Taking the time to plan on the front end will help with long-term outcomes.
WRITTEN BY SAM BLANCO, PhD, LBA, BCBA
Sam is an ABA provider for students ages 3-15 in NYC. Working in education for twelve years with students with Autism Spectrum Disorders and other developmental delays, Sam utilizes strategies for achieving a multitude of academic, behavior, and social goals. She is also an assistant professor in the ABA program at The Sage Colleges.