Many of us have heard these terms used interchangeably, but they have some important differences! Generally, we can agree that both are important… but how do we assess consent and assent?
Defining the Terms
First things first: Consent, in a basic sense, is the explicit permission for something to happen or an agreement to do something. It is most often used in legal and ethical contexts. Sometimes, consent is not able to be given by the person being cared for and must instead be given by a caretaker.
Assent, on the other hand, is a general agreement to participate. It is not limited to a verbal confirmation, but instead consists of all the verbal and nonverbal communication that could be part of an agreement (or lack thereof). Consent and assent are sometimes used interchangeably, although the difference is important.
An example of these two concepts may be a child whose parents have given consent for him to play on the playground. The child also confirmed that they would like to go outside and play; however, once the child goes outside, he hovers near the classroom door and avoids the equipment and other children. We can see in this example that while consent was secured, the child did not assent to participating. This could be for a whole host of reasons: he decided he didn’t like the heat, he misunderstood what was going to happen outside, he didn’t want to disappoint his friends. The critical element here is that we acknowledge the importance of both.
Consent and Assent in Action
In a working relationship, consent starts with a document called “informed consent.” This will include what to expect from this intervention, risks and benefits, different procedures that may be used, statements of confidentiality, and who can be included in the treatment. There may be other elements, but the goal is to make sure that everyone is on the same page for what treatment can look like. Assent is not typically included in an “informed consent” document, but is no less important.
Consent and assent should be continually assessed. How often this assessment is done formally should be included in the informed consent document; it should also be reviewed whenever a goal is achieved or the treatment plan is changed. Assent may look differently to each individual person so strong rapport is important to making sure that assent is honored.
It is important to remember that both consent and assent are necessary in all decisions throughout the day. They are super important for promoting autonomy. This may look like asking a child before touching them. If this is not an option (consider a situation where safety may be at risk), then the child should be informed of what and why an action is taking place without their permission. Close attention should be paid to their reaction and future decisions should be made with as much of their permission as possible.
About the Author
Jeridith Lord is a practicing clinical counselor and a Board Certified Behavior Analyst. Her passions include research in trauma informed care and compassionate care. She has been fortunate enough to present internationally on topics such as compassionate care in first responders, behavioral training for first responders, adherence to ethical guidelines, traumatic impact and mental health collaboration, and advocacy for domestic violence and sexual assault survivors. Jeridith is a third-year PhD student and an adjunct professor at Endicott College and Southern New Hampshire University.
Over the years, I’ve seen several behavior intervention plans written and implemented. Typically, these plans include reinforcement for the desirable behavior, but I see the same mistakes crop up again and again. Here are a few common mistakes in implementing reinforcement to look out for:
Fail to identify individual reinforcers.
Hands down, the most common error I see is identifying specific activities or items as reinforcing. For instance, many people love gummy bears, but they make me want to puke. Presenting me with a gummy bear would not increase my future likelihood of engaging in the appropriate behavior! You must account for individual differences and conduct a preference assessment of your learner, then make a plan based on his or her preferences.
Fade reinforcement too quickly.
Let’s say you’re working with a child named Harold who draws on the walls with crayon. You implement a reinforcement plan in which he earns praise and attention from his parent each time he draws on paper. The first few days it’s implemented, Harold’s rate of drawing on the wall greatly decreases. Everyone claims that his behavior is “fixed” and suddenly the plan for reinforcement is removed… and Harold begins drawing on the wall once more. I see this sort of pattern frequently (and have even caught myself doing it from time to time). After all, it can be easy to forget to reinforce positive behavior. To address this issue, make a clear plan for fading reinforcement, and use tools to help remind you to provide reinforcement for appropriate behavior.
Inconsistent with reinforcement plan.
Harriet is writing consistently in a notebook, to the detriment of her interactions with peers. Her teachers implement a DRO, deciding to provide reinforcement for behavior other than the writing. However, the teachers didn’t notify all the adults working with her of the new plan, so Harriet’s behavior persists in certain environments, such as at recess, allowing her to miss multiple opportunities for more appropriate social interaction. To address this issue, make a clear outline of the environments in which the behavior is occurring and what adults are working in those environments. Ensure that all of the adults on that list are fully aware of the plan and kept abreast of any changes.
Don’t reinforce quickly enough.
This one can be quite challenging, depending on the behavior and the environment. Let’s saying you’re working with a boy named Huck who curses often. You and your team devise a plan to reinforce appropriate language. You decide to offer him tokens that add up to free time at the end of the school day. However, sometimes as you are handing him a token for appropriate language, he curses again right before the token lands in his hand. Though it was unintentional, the cursing was actually reinforced here. Remember that reinforcement should be delivered as close to the desired behavior as possible. To address this issue, consider your environment and materials and make a plan to increase the speed of delivery.
Fail to make a plan to transfer to natural reinforcers.
Ultimately, you don’t want any of these behaviors to change based solely on contrived reinforcement. Making a plan for reinforcement of appropriate behavior is essential, but your ultimate goal is to have the behavior be maintained by naturally occurring reinforcement. To address this issue, the first thing you need to do is identify what that naturally occurring reinforcement might be. For Harold, it might be having his artwork put up in a special place or sharing it with a show and tell. For Harriet it might be the interactions she has with peers on the playground. Once you have identified those reinforcers, you can create a plan for ensuring that the learner contacts those reinforcers over time. This might include pairing the naturally occurring reinforcers with the contrived reinforcers, then fading out the latter.
Ultimately, it’s important to remember that reinforcement is not as simple as it seems. Taking the time to plan on the front end will help with long-term outcomes.
WRITTEN BY SAM BLANCO, PhD, LBA, BCBA
Sam is an ABA provider for students ages 3-15 in NYC. Working in education for twelve years with students with Autism Spectrum Disorders and other developmental delays, Sam utilizes strategies for achieving a multitude of academic, behavior, and social goals. She is also an assistant professor in the ABA program at The Sage Colleges.
You probably get a lot of questions from families about different kinds of interventions, diets, supplements, experimental treatments, etc. It can be stressful to know how to answer these questions. As behavior analysts, we’re experts in behavior science and we’ve been taught to prioritize evidence-based practices for our clients. Does that mean that families should be discouraged from trying different strategies that are outside of behavior science? Of course not (provided those different strategies are safe). It is important that we understand how to integrate and understand these strategies within the context of the support we’re providing.
While behavior analysts can’t provide recommendations about non-behavior analytic interventions, we can support families in trying safe strategies using a scientific approach. We can help the family identify what kinds of outcomes they’re hoping to see and data collection strategies to help understand the impacts. We can help families interpret information and understand what is being marketed to them.
We can utilize the same scientific process with any strategy and help parents make informed decisions about the interventions they’re trying. Let’s go through an example together.
Let’s say that a family comes to you saying they want to try a new dietary supplement, and their pediatrician has already approved its use. You’ve heard of it but don’t know much about it. As far as you know, there isn’t research to demonstrate any benefits for children but no research indicating red flags either. You tell the family that providing advice about supplements is outside of your scope of practice, but you’d love to help them come up with a data collection system to help examine the effects.
This is great time to talk to the family about what their expectations are about the supplement and what they’re hoping will change because of introducing it to their child’s diet. Here are the steps:
Identify the intended outcomes. Help families identify specific behaviors they can track that will be indicators of if the goals are working. Remember, we can’t track happiness but we can help families think about what behaviors their children do to show they are feeling happy.
Develop a data collection system. Remember that this data collection system will be used by the families, not a behavior technician. The simpler and more feasible the structure is for data collection, the more likely you are to get accurate data. In my humble opinion, I would prioritize accurate data over robust data in these instances
Identify some criteria. Talk to the family about what kinds of results they’re looking to see and how they’re going to know whether the supplement is working. What is the timeline for evaluating the data and seeing the progress? What are the numbers we’d need to see in order to consider it a success? What would be the criteria for immediate discontinuation of the supplement?
Collaborate with other providers that support the family. Medical doctors can provide important context about medical considerations and may be able to provide insight on important behaviors to track. School staff can help provide context about how the child is doing at school. Everyone is an important part of the team!
About the Author
Nahoma Presberg, MS BCBA NYS-LBA, is a Board Certified Behavior Analyst. Nahoma obtained their master’s degree at the University of Rochester in Human Development. They have been working with clients in their homes for the past 6 years but has over a decade of experience supporting children with developmental disabilities. Nahoma is passionate about neurodiversity affirming care and thoughtful programming that helps every client thrive.
This month’s ASAT feature comes to us from Shira Karpel, MEd, BCBA and Shayna Gaunt, MA, BCBA, How to ABA. To learn more about ASAT, please visit their website at www.asatonline.org. You can also sign up for ASAT’s free newsletter, Science in Autism Treatment, and like them on Facebook!
I am a first-year teacher in a self-contained classroom. I appreciate how data can guide my decision-making and help me better assess progress. Nonetheless, I feel a bit overwhelmed and would welcome some general guidance on what type of data to collect and when.
Thank you for your question. We are happy to hear you are considering data-based decision-making to best assess your students’ progress. As ABA professionals, data collection plays an essential role in making decisions and updating or revising programs based on what the data tells us. However, it is possible to be so consumed with data that it interferes with teaching. How well can a person engage and think on their feet when they are preoccupied with data collection? It can also be challenging to select the right method of data collection to accurately reflect skill progress (or lack thereof). For instance, it may look like a student is not mastering any goals, when, in fact, a different type of data collection method may tell a different story.
Data plays a very important role in the classroom for students who have Individualized Education Plans (IEP). In developing an IEP, goals should be chosen based on assessments, as well as what will be personally meaningful to the student in that setting. Data collection is a vital tool in the classroom. It is necessary to assess a student’s strengths and areas of support which will then inform potential goals. For example, data from an assessment can tell us that a student is currently able to label numbers 1-5 and based on this, we might propose a goal of labeling numbers 1-10. Think about the end goal in observable and measurable terms and then choose a type of data collection that is doable amidst a busy classroom. Then, we will be able to make data-based decisions, share objective assessments of progress and update IEPs accordingly. It all sounds nice but how can we use data without it becoming overwhelming?
We feel strongly that data should only support learning and never impede it. This is why it is important to choose a method of data collection that allows teachers to a) monitor progress, b) be present in the moment, c) engage with their students, and d) remain focused on teaching. Students will learn more from good teaching than from good data. In a classroom, this often means that you would choose methods of data collection that are manageable when teaching a large group.
Let’s review a few of our favorite data-collection methods and their potential applications in the classroom.
Frequency
Frequency refers to the number of responses within a specific period of time. In other words, how many times are you seeing the occurrence of a particular target? Tally counters are a great way to collect frequency data. They are not cumbersome! A tally counter is something you can wear on your finger or waist while you’re teaching and click the counter when you observe a behavior. Frequency is often a common measure for behavior reduction goals, for example reducing the number of times a student elopes from the classroom. Frequency data are often collected as part of toilet training efforts (e.g., successes, accidents, initiations). However, frequency is also a simple measure for a lot of skill acquisition goals. Requesting and spontaneous language are some programs where we may choose a frequency count over any other type of data collection. For example, how many times a student greeted a friend or how many times a student asked for help. There can be creative ways to keep track of frequency, most teachers I work with love to carry around a sticky note and make tallies when they can! These tallies can then get added up at the end of the day and graphed.
Duration
Duration refers to how long the behavior persists. We often take duration data when we want to know how long it takes students to complete specific tasks. We also take duration data when analyzing impeding behavior, like tantrums. How long do they persist? It’s important to include duration data for interfering behavior because it can be an important measure of progress; frequency may stay the same but duration increasing or decreasing is meaningful. Duration can also be used for skill acquisition goals like time on task or social skills.
An efficient way to track these interfering behaviors is to use partial interval recording. By dividing the observation period into smaller units of time, like 1-minute and then checking off the times that these behaviors occur, we get information about both duration and frequency. This can then be graphed so that we can see trends in behavior.
Probe Data
Probe data means that we take yes/no data on the first trial of a program and then put our pencils down and teach! Probes can also be done less often if in a classroom situation (e.g., think spelling test), or in the community. Teaching should still happen after the probe (especially if it was incorrect!). Mastery may be something like “3 correct responses across 2 different people.” For example, if a student is learning to label colors, you might mark down a “yes” or “no” for the first time each day that you ask them to name their colors. Then, continue to do lots of fun play activities with colors (but no data!). Probe data can be great for progressing students who learn quickly through programs. They may only need a few exposures of the material. For example, a probe data sheet can be used with a program like, “Expressive Labels” such that multiple targets can be run simultaneously, and the student can advance through them quickly. Caution: the downside of probe data collection is that instructors might not run as many teaching trials as they should if there are no data to record after the first response. Probe data can be easily achieved in a classroom setting as there is often a lot of teaching happening anyway throughout the day.
Trial-by-Trial Data
Taking trial-by-trial data means that we record data for each trial run and then get a percentage of correct responses. If a student is asked to label a set of 3 colors (e.g., blue, red, yellow), you can take data on each color presented (correct or incorrect) and end up with a percentage score. Mastery is usually something like, “80% or more for 2 sessions, across 2 people.” Some children need more exposure, and repetition is good for their learning. Collecting trial-by-trial data encourages instructors to run at least 10 trials. Graphing the percentage tells us more information about performance across trials than probe data. It is also more objective than rating scale data. By graphing the percentage, we can see if the curve is increasing or decreasing or if there are any other notable changes.
See the example below for one graph illustrating an increasing trend and one graph illustrating a decreasing trend. The graph with increasing data tells us that the student can label all 3 of those colors with proficiency. When a graph looks like this, we can “master” teaching those 3 colors and move to teaching another set of colors. The graph with decreasing data tells us that we need to look closer at how the colors are being taught as the student is not learning the way we are teaching. Perhaps the student has over-generalized and is answering, “Blue” for every answer, or perhaps the student is just randomly selecting a response, or just not motivated to respond. In any case, the data show us that we need to look at our teaching procedures and make changes.
Figure 1. Graph with an increasing trend.
Graph with a decreasing trend.
This is often the default measure of progress but also the most cumbersome because it means that you are also looking for every opportunity that the response could have occurred but did not. Percentage is most appropriate for testing-style goals – when working at a table and the student is clearly presented with multiple opportunities in a row. For example, after a unit on animals, the teacher presents 10 animals for the student to label. The student’s score out of 10 would be the percentage correct. This is often not ideal for many goals, so think about choosing frequency or probe instead.
Rating scale data
A rating scale describes behavior along a continuum, like a rubric. Although rating scale data can be subjective, they can describe the level of independence (or resistance) for an activity without impeding teaching. During the time when the instructor and the student are getting to know each other, relationship building and engagement (a.k.a. pairing) are first and foremost (Oliveira & Shillingsburg, 2023). A clipboard or electronic data collection may ruin the quality of that interaction. Rating scale data can outline some goals for the instructor to work on and then the child can be rated at the end of the session, based on a continuum of how well they did that day. The scores are then graphed. Check out more about rating scale data sheets and download a free copy.
A rating scale is also a great measurement tool for group-based learning in a classroom. The students can each have goals that can be accomplished in a group setting, for example “staying on task” or “raising hand.” Then, while the teacher is teaching, another staff member can record rating scale data. Rating scale data is also something that doesn’t need to be recorded in the moment; when the activity is over, the teacher can recall how the student did based on the defined scale. Rating scale data are easy for any staff member to collect without it being overwhelming.
Conclusion
Choosing a data collection method is an important part of the process but only the first step. Do not forget to then analyze and refer to the data to make data-based decisions. Include your team in reviewing the data and ask for input as to what they think might need to be changed. Refer to data when dialoguing with parents about progress, particularly if parents were part of the data collection. You want them to appreciate that data tell an important story.
As a teacher, you want to see your students make progress. Data can help you assess, plan, and monitor that progress in a way that doesn’t have to be overwhelming. When used as a tool, it will help you, parents, and the student see that progress and be able to make changes accordingly.
References
Baer, D. M., Wolf, M. M., & Risley, T. R. (1968). Some current dimensions of applied behavior analysis. Journal of Applied Behavior Analysis, 1(1), 91. https://doi.org/10.1901/jaba.1968.1-91
Burke, M. D., Vannest, K., Davis, J., Davis, C., & Parker, R. (2009). Reliability of frequent retrospective behavior ratings for elementary school students with EBD. Behavioral Disorders, 34(4), 212-222. https://doi.org/10.1177/019874290903400403
Chafouleas S. M., Christ T. J., Riley-Tillman T. C., Briesch A. M., & Chanese J. A. M. (2007). Generalizability and dependability of direct behavior ratings to assess social behavior of preschoolers. School Psychology Review, 36(1), 63-79. https://doi.org/10.1080/02796015.2007.12087952
Cooper, J. O., Heron, T. E., & Heward, W. L. (2020). Applied behavior analysis. Pearson UK.
Fiske, K., & Delmolino, L. (2012). Use of discontinuous methods of data collection in behavioral intervention: Guidelines for practitioners. Behavior Analysis in Practice, 5(2), 77-81. https://doi.org/10.1007/BF03391826
Iovannone, R., Dunlap, G., Huber, H., & Kincaid, D. (2003). Effective educational practices for students with autism spectrum disorders. Focus on Autism and Other Developmental Disabilities, 18, 150-165. https://doi.org/10.1177/10883576030180030301
Merbitz, C. T., Merbitz, N. H., & Pennypacker, H. S. (2015). On terms: Frequency and rate in applied behavior analysis. The Behavior Analyst, 39(2), 333-338. https://doi.org/10.1007/s40614-015-0048-z
Oliveira, J., & Shillingsburg, A. (2023). Clinical Corner: Building rapport with students using specific strategies to promote pairing. Science in Autism Treatment, 20(12).
Citation for this article
Karpel, S., & Gaunt, S. (2024). Clinical Corner: How do I choose the right data collection method? Science in Autism Treatment, 21(5).
About the Authors
Shira Karpel, MEd, R.B.A (Ont), BCBA is the co-founder and director of How to ABA, an online resource and community for ABA professionals. Shira has a Masters in Special Education and has been in the field of ABA since 2011, receiving her BCBA in 2014. Together with Shayna, they trained and taught many therapists, clients, and parents and collected a massive bank of ABA programs and resources. In an effort to give back to the field, Shira and Shayna decided to create How to ABA as a way of sharing our collection of resources with others. As a former teacher, her passion is in using ABA in classrooms in order to create positive and comprehensive learning environments for all students. She is the Clinical Director at a private school in Toronto and is loving getting to make a difference in the lives of children and families daily. She is passionate about making the principles of ABA practical, doable and relevant to every child in any situation
Shayna Gaunt, MA, R.B.A (Ont), BCBA is a dedicated professional in the field of Applied Behavior Analysis (ABA) and co-founder of How to ABA, an online resource and community supporting ABA professionals. With over two decades in the field, a Master’s Degree in ABA from the University of Nevada Reno, and extensive international experience, Shayna brings a vast expertise across diverse settings. She emphasizes collaborative excellence in direct therapy, supervision, and training, striving to deliver high-quality services and resources to clients and fellow ABA practitioners. Through How to ABA, Shayna aims to make ABA principles accessible and practical, fostering a community where professionals can share, learn, and grow together.
By Ashleigh Evans, MS, BCBA, reposted from the Different Roads Archives
Children with autism and other neurodivergence commonly struggle with transitions. The shift from summer to the start of a new school year is one of the most challenging transitions. Getting back into a new routine is not easy and often requires support and patience through these changes. Behavior analysts play a vital role in helping these children navigate the back-to-school season. Let’s review four strategies you can try to make for a successful back-to-school transition for your clients.
1. Maintain Open Communication with School Staff
Open communication between the ABA and school teams can help smooth the transition. Introduce yourself to your client’s teacher and support staff, communicating your desire to collaborate for your shared learner’s best interests. Use this as an opportunity to also share and celebrate your client’s growth during the summer. Share mastered skills that your client achieved over the summer and any new concerns to help the school team gain an updated picture of their current skills and behaviors.
2. Review and Update Goals
Take a look through your client’s goals and progress made. The ultimate goal of ABA is to prepare our learners for optimal functioning in the least restrictive environments. Consider updating goals to encourage the development of skills that will help them be more successful at school. If they attended school last year, review their IEP and reflect on areas they struggled with in the previous year.
One area to consider is your learner’s self-advocacy skills. Do they have the necessary skills to express their needs and desires in a manner that school staff can understand? Do they have the ability to communicate when something is uncomfortable, they need a break, or someone is bothering them? These skills are all critical for success in school and onward. Ensure goals are in place to teach these skills, if not already mastered.
3. Increase Caregiver Training and Support
During times of major transitions, parents and caregivers may also struggle to navigate the routine shifts that often come with behavioral changes in their child. Empower your client’s parents to support their child through this shift by enhancing caregiver training. If clinically appropriate and feasible, increase caregiver training sessions before and for the first few weeks after the school year starts. Providing additional support can set everyone up for success.
4. Implement New Antecedent Strategies
Consider the antecedent strategies you can implement to help your client better cope with the new routines and expectations. Visual supports, such as a visual schedule with the child’s morning routine or daily schedule, can help your client envision what comes next, making it easier for them to get into the swing of things. If your client enjoys social stories, you can create one to review with them (or have parents read it to them) to familiarize them with what to expect. Make sure it’s personalized and unique to them with components such as their teacher’s name and picture.
Plan Ahead for a Successful School Year
The back-to-school season can be a stressful time for children and their families. However, with caregiver planning and support, behavior analysts can help make this process significantly easier. Help your families navigate change and prepare for a year of success at school by trying the aforementioned strategies. Each client is unique, so as always, tailor your approach to their particular needs and preferences.
About the Author
Ashleigh Evans, MS, is a Board Certified Behavior Analyst. She has been practicing in the behavior analysis field for over 13 years and opened her own independent practice in early 2022. Her experience has been vast across different age groups, diagnoses, and needs. She is passionate about improving the field through education, reformative action, and better supervisory practices, leading her to create content and resources for families and ABA professionals which can be found on her website, www.abaresourcecenter.com
By Sarah Kupferschmidt, MA, BCBA. Reposted from the Different Roads Archives
I am passionate about empowering children with special needs and their families with skills and knowledge that they can use to improve their quality of life. This is why I am super excited to be sharing tips and strategies that relate to keeping your child with autism safe on the street. Learning to navigate the real world involves a lot of complex skills that we sometimes take for granted. For example, learning to determine when it is safe to cross the street requires the ability to attend to your environment, the ability to identify moving cars from cars that are still, the ability to identify the signal at the cross walk that lets you know it is safe to cross, among many, many, more. In some cases even more advanced problem solving is required because if the sign says it is safe to cross and a motorist continues through the intersection we need to be able to identify the moving car is approaching and that we need to wait for it to pass before crossing the street. So where do we begin?
Tip #1: The Learner is Never Wrong
I love the saying “the learner is never wrong” because of what it implies. Whenever considering teaching a new skill to a child or student we need to focus on that unique child’s strengths and weaknesses. Where do we need to boost up their skills and what do they already know so that we can capitalize on those strengths. Before going out to teach your child with autism how to cross the street safely, they should have some imitation skills, be able to respond to instructions and attend to you or a teacher amidst a lot of distractions (e.g., cars, background noise and pedestrians, just to name a few). Once you have determined they are ready to learn this important skill you would want to use things that are of interest to them and that you know align with their learning style. For example, are they a visual learner and if so, how can you incorporate visuals to maximize their learning potential in how you go out and practice crossing the street safely?
Tip #2: Simplify the Complex Skills
As mentioned earlier in the post, many of the skills that we use actually have many components, something we take for granted. In this case, teaching how to cross the street might involve the following steps:
Stop at the curb/crosswalk
Look at the crosswalk signal
Decide if it is safe to cross (e.g., does it say ‘walk,’ or does it say ‘stop’)
If the sign says walk, then look both ways
Decide if it is safe (e.g., is there a car moving or not)
Walk safely across the street (e.g., this means walking not running, perhaps holding your hand)
It is important to remember that these steps are just an example of what you might teach. You would individualize this based on the environment in which you live (e.g., if there is a crosswalk sign or crossing guard, or not) and the expectations you have as a family (e.g., to hold the hand or not). Teach this using tools that you know are effective with your unique child. For example, you may decide to print out a visual depiction for each of the steps and show them as you talk about it and practice. This depends on your child’s unique learning style. As with every skill that that we teach, it is never enough to just tell someone or show someone how to do it. We need to actually go out and practice.
Tip #3: Practice, Practice, Practice
Use every opportunity that you have to go out and practice this very important skill. I would also recommend that you set up specific times to go out and practice. You can use the visuals that you printed and go through each of the steps while you are out. If you notice that your child is struggling on a particular step, then practice that particular step at home even more. For example, if your child is not identifying the walk signal when you are out on the street, set up times to go over that at home.
Tip #4: Monitor Progress
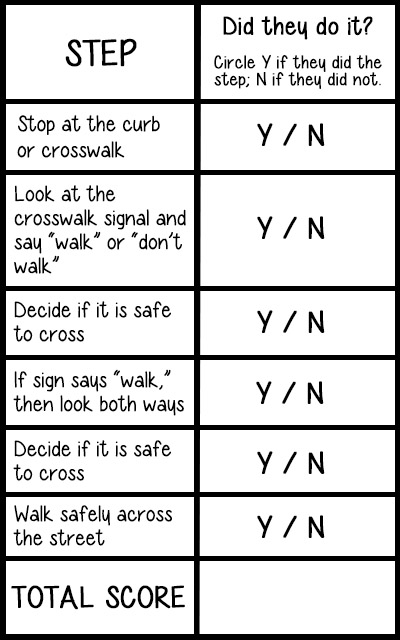
In order to see how your child is doing on each of the steps it is a good idea to record how they do on each of the steps. You might print off a checklist with each of the steps that looks something like this:
You would calculate the number of times you recorded a Y over the total number of steps (e.g., in this case 6). For example, if I worked on this with my child and he did all of the steps he would get a 6/6. If he missed a step his overall score would be 5/6 or 83%. This score can then be used to monitor progress. I would also suggest that anytime you go out and practice you highlight whichever step(s) that they missed, if any. This will allow you to see if you need to work on something a little bit more before you go out and practice.
Tip #5: Notice the Good Stuff
Feedback is critical when you are teaching a new skill. Otherwise how is your child going to know how they are doing? This means that when they get it right we need to notice it and we need to be specific about what it is they did well. You can even use the visuals if you have them. You might say something like “I love the way you followed all of the steps of what to do when crossing the street safely! You stopped at the curb, looked at the signal…etc.” You may point to the visual as you tell them. If they missed a step remind them that next time they should try to remember what it is that they missed. Anytime they do one of the steps spontaneously, point it out to them and give lots of praise. Over time we can fade the praise out but it is really important when teaching a new skill, especially at the beginning.
About the Author
Sarah Kupferschmidt, MA, BCBA, is a Board Certified Behavior Analyst (BCBA) who has worked with hundreds of children with autism and their families across Ontario. She has had the privilege of supervising ABA programs and training clinical staff in those programs. Currently Sarah offers parent coaching and workshops to teach parents but also educators on the most effective ways to teach children using the principles of ABA. She is also a part-time faculty member at Mohawk College in the Autism Behavioral Science program, in the social sciences program at McMaster University, and an Adjunct Professor at Sage Graduate School. Sarah has appeared as a guest on CP24, CHCH news, Hamilton Life and the Scott Thompson radio show as an authority on autism.
The transition back to school and back to a new routine is always an exciting, yet bittersweet time for students and educators. Carefree summer days are in the past, and getting back into a structured daily routine can be an overwhelming process. However, new teachers, new friends, and new settings provide the opportunity to make progress with academic, behavior, and social goals. Even while students and their families should enjoy every precious moment of summer fun, it is also important to set aside some time to prepare for the transition in the new school year.
Getting Proactive
Most school-based BCBAs can attest that the most important aspect of school consultation is assisting educators and other stakeholders to be proactive about behavior instead of reactive. This advice is especially valuable while preparing for a new school year. Teachers and families can begin to discuss and implement proactive strategies in the days prior to the first day of school.
For teachers and school based BCBAs, summer preparation days can be used to discuss simple environmental manipulations that can be made within the classroom. For instance, before students even step foot in the classroom, the teacher and other support staff can arrange seating that is limited from distraction and enhances engagement. A common suggestion from BCBAs is usually to seat students with a history of elopement behavior far away from the exit doors. Some consultants may even suggest preparing some visual supports and schedules ahead of time in order to prepare staff and students. Students thrive with structure and organization, so if the classroom has established expectations the students will find it easier to decide which behaviors lead to rewards and desired activities.
Building Rapport
Antecedent interventions do not only apply to teacher prep days. Chances are, not all students will engage in challenging behaviors on the first day of school. Hence, those first days of school are crucial because they are the opportune times for pairing. Classroom staff should prioritize gaining trust and rapport with students. This process can begin the moment the students arrive at school on the first day. Teachers and staff can begin pairing with students simply by greeting students with a smile and limiting demands. Students should be given the chance to feel happy and relaxed while adjusting to a new environment.
The more the students feel comfortable in the environment, the more likely they are to view the adults in the environment as a reinforcer, or a signal for access to preferred items and activities. When trust and rapport is established, it will also be easier for teachers and staff to engage in activities that may not be highly preferred. Of course the primary focus of the teachers should not be to place increasingly difficult demands on the students. However, establishing themselves as a person that will provide rewards and other motivators, allows the adults in the classroom to assist the students in developing pivotal behaviors that will provide access to a whole world full of reinforcing items and activities.
While students are adapting to the new enrichment, teachers and staff can use the opportunity to informally assess the students’ preferences. Enriching the enrichment with items high on the students’ preference list will not only assist in the pairing process, but can also be used as potential motivators for instances of positive reinforcement scenarios.
Embracing Collaboration
Lastly, the most important aspect of the transition back to school and adjustment to a new environment and routine is collaboration with all key stakeholders. Parents and caretakers, as well as teachers, should be involved and have input on any strategies and goals put in place. The more the students’ parents and caretakers feel involved in the decisions being made for their children, the more likely they are to carry out plans with fidelity. Also, establishing effective collaboration and communication assists with overhaul generalization of behaviors and makes the students’ support system stronger and more successful.
About the Author
Alicia Marshall, MAT, BCBA LBS, started out as a Special Education teacher and made the switch over to full-time BCBA 5 years ago. Alicia received her BCBA coursework at Rutgers and currently works as a Director of Behavioral Health in the Greater Philadelphia area. Alicia is passionate about making learning fun for all stakeholders and to encourage educators to focus on socially significant goals and compassionate care.
When Alicia is not disseminating the science of ABA, she can be found on the beaches of the Jersey Shore (and occasionally Hawaii) with her husband and two dogs.
WH questions are essential building blocks of communication. Understanding and responding toquestions about who, what, when, where, and why is vital for a child’s language development. BCBAs and educators commonly focus on teaching these pivotal skills for many reasons. Let’s explore why teaching WH questions is important and how it can help shape a child’s language and communication skills.
What are WH Questions?
Before we dive into why WH questions are important, let’s consider what WH questions are. WH questions encompass many different questions that start with the words “who,” “what,” “when,” “where,” and “why. While it doesn’t start with WH, some people also group “how” questions under this umbrella. WH questions include the following.
Who Questions–Questions about people, such as “Who is coming over today?”
What Questions–Questions about things, thoughts, actions, or ideas, such as “What did you think about that movie?”
When Questions–Questions about times, days, or dates, such as, “When is your birthday?”
Where Questions–Questions about places, such as, “Where did you go last night?”
Why Questions–Questions about the reasons or causes for things, such as, “Why do I have to cut the grass?”
It’s important to teach kids to both ask and answer who, what, when, where, and why questions as they navigate their home, social, and academic environments.
Why is it Important to Teach Kids to Answer WH Questions?
There are many reasons why children should be taught to answer WH questions, including the following.
Safety–If a child is ever lost or in another unsafe situation, they may need to communicate critical information, such as, “What’s your name?” “Where do you live?” “Who are your parents?”, etc. It can also provide parents peace of mind when their child can answer key questions about their day.
Building friendships and social engagement–Answering WH questions allows a child to engage socially with peers and build meaningful relationships.
Academic success–Understanding how to answer WH questions is vital in educational settings, where children are expected to communicate their knowledge through reading comprehension, math equations, and many other subjects.
Reciprocating conversations–Answering WH questions helps learners develop conversational skills, including answering and reciprocating questions. This is necessary in many settings, including social, educational, vocational, and at home.
Memory and recall–Teaching children to answer WH questions is a pivotal skill that leads to additional skills, such as recalling events.
Why is it important to Teach Kids to Ask WH Questions?
Learning to ask WH questions is equally important as answering them. Let’s explore some pivotal reasons that underscore the significant benefits of teaching children to ask WH questions.
Understanding the world around them–Asking WH questions encourages curiosity, fostering an understanding of the world around the child.
Academic success–An ability to ask questions aids in academic success, as the child takes an active role in their education by questioning things that expand their knowledge.
Initiating conversations–Teaching children to ask WH questions helps them develop conversational skills, including initiating conversations. This can foster meaningful connections with peers and others in their lives.
Problem-solving–Children who can ask WH questions can build upon their knowledge, asking questions that promote critical problem-solving skills.
Resources for Teaching WH Questions
Teaching children with autism and other neurodevelopmental differences to ask and answer WH questions is a complex process with many layers. Many WH questions are abstract, involving time (when questions) or cause and effect (why or how). These can be challenging concepts for neurodivergent children to grasp.
The first step is to teach simple labeling (referred to as tacts inverbal behavior language). Labeling items and activities is a necessary prerequisite skill. For example, before a child can answer the question, “Where is your cup?”, they need to know how to label items, such as “couch,” so they can answer by saying “on the couch.” You can useflashcards to teach your learner to label various objects, including common objects around the home and school, food, clothing, body parts, and more.
As children develop the basic prerequisite WH skills, you can make learning fun and engaging by expanding upon their knowledge through games and activities.The Ask & Answer Social Skills Game is one such engaging game that you can play to help your learners develop skills related to answering WH questions.
Ashleigh Evans, MS, is a Board Certified Behavior Analyst. She has been practicing in the behavior analysis field for over 13 years and opened her own independent practice in early 2022. Her experience has been vast across different age groups, diagnoses, and needs. She is passionate about improving the field through education, reformative action, and better supervisory practices, leading her to create content and resources for families and ABA professionals which can be found on her website, www.abaresourcecenter.com
ABA often gets a bad rap due to misunderstandings about reinforcement. In my career alone, I’ve had people tell me that people are not like rats and pigeons, that reinforcement harms intrinsic motivation, and that when I do produce behavior change, it has nothing to do with ABA but with my abilities as a teacher. Today, I’d like to clear up some misconceptions about reinforcement.
Reinforcement is not equivalent to rewards.
Reinforcement is anything that occurs immediately following a behavior that increases the future likelihood of that behavior. For instance, I am more likely to say hello to my neighbor down the street because in the past he has responded by saying “hello” back to me. However, I do not say hello to my next-door neighbor because she has never responded to my greeting. My history of reinforcement with the neighbor down the street increases the likelihood that I will greet him upon seeing him.
Reinforcement occurs in the natural environment all the time, whether we are conscious of it or not.
We are reinforced by paychecks for going to work, by our favorite dessert for visiting a restaurant 30 minutes out of our way, by compliments when we get a new haircut and more. ABA utilizes reinforcement when an individual is not acquiring skills in order to help them learn. And when ABA is implemented correctly, reinforcement should be as close to naturally occurring reinforcers as possible and should be reduced systematically over time to levels that would naturally occur in their environment.
Reinforcement works for dogs and for humans.
The previous two points illustrate that humans do respond to reinforcement, and decades of scientific research back that up. Comparing the work behavior analysts do with humans to the work behavior analysts do with other animals is not far off base. What is off base is using such a comparison to imply that behavior analysts treat people with disabilities like dogs. As with other professionals who work with individuals with disabilities, (such as speech therapists, physical therapists, nurses, etc.) most behavior analysts are professionals who put a lot of time, care, and love into their work.
Reinforcement is individualized.
Everything we do in ABA is individualized because human beings are wonderfully complex creatures that cannot be characterized by statistics, averages, or norms. One of my students may find stickers reinforcing; another may show no interest. One student may find listening to music reinforcing; another may cover his ears and ask me to turn it off. In ABA, we seek to find the items and activities that are motivating for individuals; then use those as tools not only for reinforcement but for increasing skills and broadening interests and opportunities. In an ideal ABA session, my students spend a lot of time engaging with items and activities that they enjoy while also learning and growing.
It’s easy to fall prey to misconceptions about reinforcement, but such misconceptions can make it impossible for us to understand how to alter the environment in order to provide the best possible outcomes for our students. As Skinner put it, “The ideal of behaviorism is to eliminate coercion: to apply controls by changing the environment in such a way as to reinforce the kind of behavior that benefits everyone.”
Sam is an ABA provider for students ages 3-15 in NYC. Working in education for twelve years with students with Autism Spectrum Disorders and other developmental delays, Sam utilizes strategies for achieving a multitude of academic, behavior, and social goals. She is also an assistant professor in the ABA program at The Sage Colleges. You can read more of Sam’s posts for DRTL here!
This month’s ASAT feature comes to us from Shira Karpel, MEd, BCBA and Shayna Gaunt, MA, BCBA, How to ABA. To learn more about ASAT, please visit their website at www.asatonline.org. You can also sign up for ASAT’s free newsletter, Science in Autism Treatment, and like them on Facebook!
I’m a newly certified behavior analyst working in a school-age program. Many of my students struggle with emotion regulation. However, my coursework and supervision were primarily focused on easily measurable, observable behaviors. While I was taught that behavior analysis doesn’t discredit private events, I just don’t know where to start. A few initial topics or tools for teaching emotion regulation would be helpful to get me started.
A Brief Review of Emotion Regulation
We cannot ignore that children have emotions. As behavior analysts, we are trained to study behavior that is observable and measurable – not private events like thoughts and emotions. But how can we ignore that some of the students we work with are struggling with managing how they are feeling? We need to allow our students to have these emotions, but it is also important to teach them coping strategies and emotion regulation techniques. In terms of social significance, this is a big one!
Individuals with ASD have more emotion regulation difficulties and consistently demonstrate less adaptive regulation strategies, as well as internalizing problems such as anxiety and externalizing problems such aggression (Cai et al., 2018). Emotion regulation is the ability to do hard things despite some uncomfortable feelings. It’s the ability to use strategies in dealing with emotions like disappointment, frustration, and anger – and being able to recover. It’s a form of resilience that many of our learners would benefit from learning.
Yes! As behavior analysts, we only implement strategies and programs to address emotion regulation that are evidence-based.
Yes! We need to be able to describe these behaviors in ways that are observable and measurable.
Yes! We need to continuously take data and analyze the data to make any necessary changes.
According to Skinner (Verbal Behavior, 1957), private events are considered behaviors that are under the control of environmental stimuli and can be defined in behavioral terms. Skinner noted that radical behaviorism “does not insist upon truth by agreement and can therefore consider events taking place in the private world within the skin. It does not call these events unobservable” (Skinner, 1974, p. 16).
In line with Skinner’s definition, emotions, and emotion regulation are private events. They are under the control of environmental stimuli, but they can be defined and measured. Let’s take ‘anxious’ for instance. ‘Anxious’ should be individually defined for each person, including observable and measurable events like flushed cheeks, red ears, and ringing of one’s hands in a particular way. Likewise, emotion regulation could be defined as using strategies like counting backward or taking three deep breaths.
So, how can we talk about feelings and teach emotion regulation strategies in a behavior-analytic way? Before we review 7 of our favorite strategies, it is very important to collect some baseline data on common triggers and setting events as these situations will inform your practice sessions and your efforts to promote generalization of the regulation skills being targeted.
7 Strategies for Emotion Regulation
The strategies for emotion regulation are best taught when a student is calm, and supported and modeled while their emotion experience is occurring. Then, it can be generalized to times when the student is more dysregulated. We don’t know about you, but when we are very upset, it only makes us feel worse when someone tells us to “calm down” or “relax.” During the heat of the moment, we’re not thinking straight. Find a moment when the student is calm and make learning into a positive experience. Here are some teaching techniques:
Identify and Teach Prerequisite Skills: Teaching emotion regulation in ABA requires foundational skills such as basic communication (i.e., the ability to get one’s needs met), understanding reinforcement (i.e., the first/then contingency), impulse control, self-awareness, and the ability to recognize emotions in oneself (Conallen & Reed, 2016). Building these prerequisite skills is necessary to ensure that learners can understand more complex concepts when you begin to teach emotion regulation strategies.
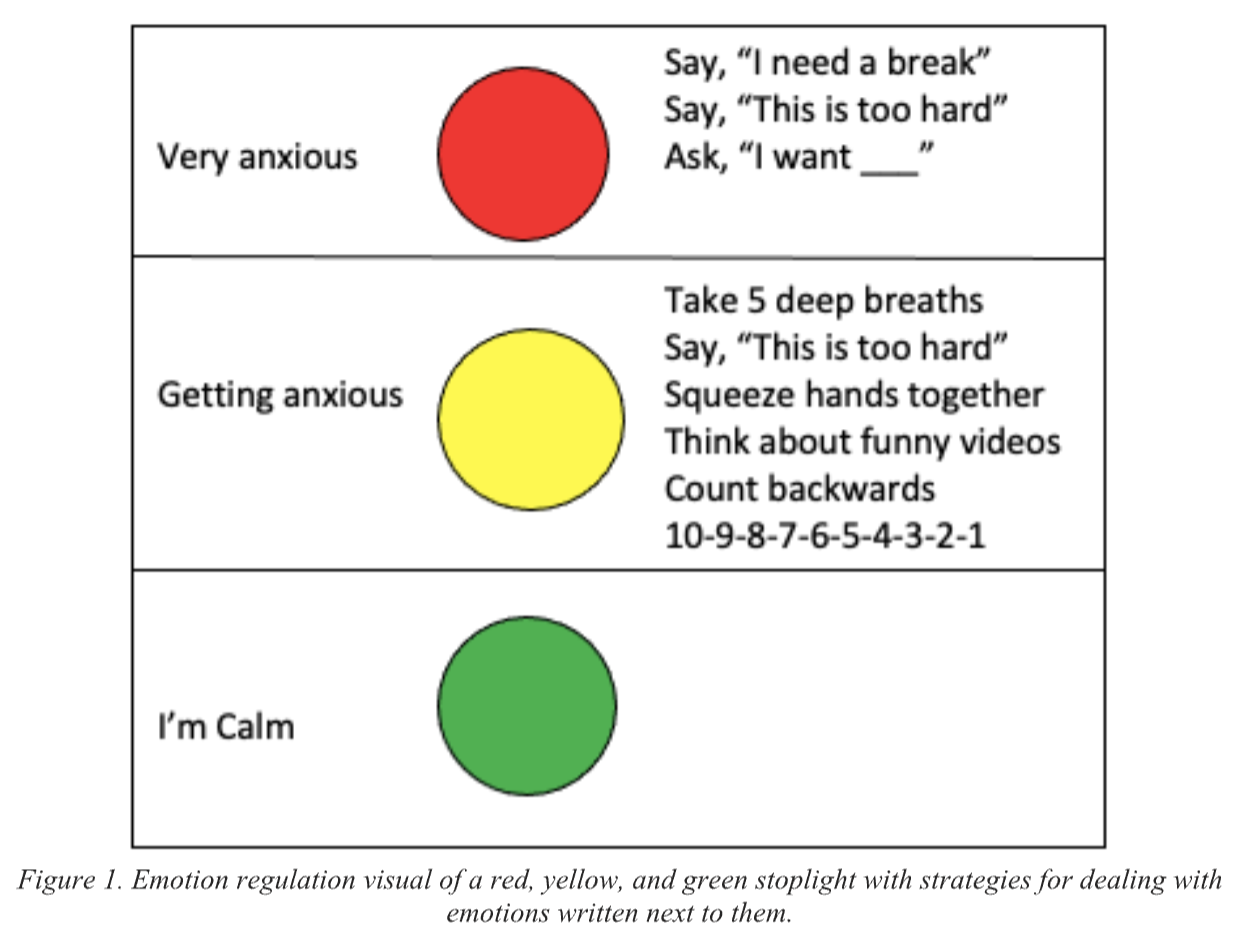
Teach Using Visuals: Visual supports, like photographs, icons, text, and video, are an evidenced-based strategy used to teach children with ASD new skills by providing cues (Hume et al., 2014). We can’t assume that a child knows what “anxious” or “frustrated” means. When teaching abstract concepts such as feelings, it is important to use visuals. Using visuals while teaching enhances understanding, supports communication, facilitates memory and recall, and increases engagement, making learning more effective and less anxiety-inducing (Beaumont & Sofronoff, 2008).There are different ways to do this depending on the age and skill of the learner. For example, you can show videos of people who are angry, anxious, and frustrated and label those videos. You can have students identify and match emotions to various situations (Conallen & Reed, 2016). Hint – for maximum success, start with emotion words that the student has already learned. Then, build in other target words that may be more accurate or nuanced from there.The stop light visual depicted in Figure 1 is an example of something that you can use to support teaching. Red, yellow, and green correspond to different emotional states. If the student can read, calming strategies can be written right beside the colors. Be sure to pair this visual with evidenced-based teaching such as prompting, modeling, and differential reinforcement. For younger students, we have used a simple flip book with small circles corresponding to different emotional states. On the front of the circles is a picture of the emotion and on the back are pictures of different calming strategies. With prompting and fading, the student can learn to flip to the color that they are feeling and then engage in calming activities. (See Figure 2 for a visual example.)
Model Labeling Behaviors: Modelling has long been used as an effective prompt in applied behavior analysis (Brody et al., 1978). Model labeling your behavior and your student’s behavior. When something happens to frustrate you, say something like, “I’m feeling so frustrated, I need to take some deep breaths to calm down.” If a student sits calmly, say, “I like how calmly you’re sitting. You look like you’re feeling green and calm,” while also pointing to the green circle. Or, if they are upset, say, “Your shoulders are raised, it seems like you’re heading towards yellow and feeling upset,” and casually flip their circle to yellow. At this point, there is no demand on the student other than to tolerate you making the comments.
Discrete Trial Teaching: In addition to labeling emotions in situ (in natural settings versus “tabletop”) using visual supports, formal teaching may need to happen. Using discrete trial teaching, teach the student to receptively identify the different colors and corresponding feelings. For example, for receptive identification, you can put out all 3 circles and say, “Show me the angry circle.” For expressive identification, you ask the student to label the emotion depicted in your materials. For example, follow up by asking, “What is this circle?”. You’ll also be asking them to label how they are feeling. “You look like you are yellow. How are you feeling?” For more on the efficacy of discrete trial teaching and some current guidelines, refer to Leaf et al. (2017). Use evidenced-based practices such as prompting, prompt fading, and differential reinforcement to teach this. With proper shaping and prompt fading, the student should eventually be able to identify and label their behavior receptively, and then expressively. To learn more about teaching receptive skills, please check out the blog on receptive labels.
Behavior Skills Training (BST): When the student is calm, use behavior skills training (Sarokoff & Sturmey, 2004) to teach positive replacement behaviors that will help regulate their emotions. BST involves four components: Instruction, Modeling, Rehearsal, and Feedback. a) Instruction: Give a brief explanation of why these calming strategies are important. If a student doesn’t understand the language, skip the wordy explanation. b) Model: Then model some calming strategies. c) Rehearsal: Practice by role playing behaviors together, such as “taking deep breaths,” “counting to 5,” “going for a walk.” etc. These may need to be individualized to the learner as you figure out what calms the student. Incorporate choice. Which techniques does your student like best? d) Feedback: Give the student lots of positive feedback, and only one piece of corrective feedback to work on. Do this a lot in practice sessions and slowly start helping the student use these strategies when they are beginning to get heightened. Initially, this task will be teacher-directed (i.e., the instructor may have to prompt the student to respond). However, the ultimate goal is to have the student demonstrate this response independently.
Give Feedback: Give the student feedback on how they’re doing. Reinforce behaviors such as “using calming strategies” or “letting others know how you feel.” It is important that praise is not given for being calm. The message should be that it is okay to feel those other emotions, it is just not okay to engage in challenging behavior when you have those feelings. If there is an episode of negative behavior where the regulation strategies were not used, debrief on that too. When the student is calm, review the incident and talk about how they can make it better next time. Use visuals for these conversations. And remember – they don’t need to be fancy. Draw it out in the moment, using stick figures and chicken scratch printing. You can visually depict the result of using the strategies and calming down versus not using the strategies. Then, you can role-play the scenario to practice how they can make it better next time.
Promote Generalization of the Skills to the Environment: Set up practice situations in novel environments and with novel people so that the student can practice using the strategies and accessing reinforcement for the behaviors they are displaying. Make sure you have visuals while you’re practicing. Look back at the common triggers that you noted during your baseline assessment. Are these new skills being used in those situations? If not, layer in practice using the above strategies so that generalization is more likely to be observed.
Measuring Progress
Data collection is also an important component of teaching emotion regulation. You should take data on things like:
Frequency of challenging behavior (it should decrease as the learner gets more proficient with self-regulation)
Duration of peak challenging behaviors from onset until offset (or until calming strategies are used)
Antecedent triggers to challenging behavior (knowing this information can guide how you teach generalization of regulation skills)
Level of independence with identifying their emotional state (i.e., how much prompting was needed, if any)
Level of independence by engaging in a calming down routine
Ability to generalize to novel environments and people
In Summary
When teaching emotions and emotion regulation, we want to first define these private events using observable and measurable terms. Then, it’s important to use evidenced-based teaching practices such as the use of visual supports, modeling, prompting, prompt fading, differential reinforcement, and behavioral skills training. Once our students have a better understanding of emotions, we want to teach our students that it’s okay to have these feelings. We want to help them understand them, express them, and then manage them. The goal is that they will use replacement behaviors such as calming techniques when they are feeling anxious, angry, etc. instead of engaging in challenging behavior. With successful teaching and practice, students can become masters of their own behavior! As a new behavior analyst, we wish you all the best!
References cited above:
Beaumont, R., & Sofronoff, K. (2008). A multi-component social skills intervention for children with Asperger syndrome: The Junior Detective Training Program. Journal of Child Psychology and Psychiatry, 49(7), 743-753. https://doi.org/10.1111/j.1469-7610.2008.01920.x
Brody, G. H., Lahey, B. B., & Combs, M. L. (1978). Effects of intermittent modelling on observational learning. Journal of Applied Behavior Analysis, 11(1), 87-90. https://doi.org/10.1901/jaba.1978.11-87
Cai, R. Y., Richdale, A. L., Uljarević, M., Dissanayake, C., & Samson, A. C. (2018). Emotion regulation in autism spectrum disorder: Where we are and where we need to go. Autism Research, 11(7), 962-978. https://doi.org/10.1002/aur.1968
Conallen, K., & Reed, P. (2016). A teaching procedure to help children with autistic spectrum disorder to label emotions. Research in Autism Spectrum Disorders, 23, 63-72.https://doi.org/10.1016/j.rasd.2015.11.006.
Hume, K., Wong, C., Plavnick, J., Schultz, T. (2014). Use of Visual Supports with Young Children with Autism Spectrum Disorders. In: J. Tarbox, D. Dixon, P. Sturmey, & J.Matson, J. (Eds). Handbook of Early Intervention for Autism Spectrum Disorders. Autism and Child Psychopathology Series. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-0401-3_15
Leaf, J. B., Cihon, J. H., Leaf, R., McEachin, J., & Taubman, M. (2017). A progressive approach to discrete trial teaching: Some current guidelines. International Electronic Journal of Elementary Education, 9(2), 361-372. Retrieved from https://www.iejee.com/index.php/IEJEE/article/view/163
Sarokoff, R. A., & Sturmey, P. (2004). The effects of behavioral skills training on staff implementation of discrete trial teaching. Journal of Applied Behavior Analysis, 37, 535-538. https://doi.org/10.1901/jaba.2004.37-535
Skinner, B. F. (1957). Verbal behavior. Appleton-Century-Crofts.
About the Authors:
Shira Karpel, MEd, R.B.A (Ont), BCBA is the co-founder and director of How to ABA, an online resource and community for ABA professionals. Shira has a Masters in Special Education and has been in the field of ABA since 2011, receiving her BCBA in 2014. Together with Shayna, they trained and taught many therapists, clients, and parents and collected a massive bank of ABA programs and resources. In an effort to give back to the field, Shira and Shayna decided to create How to ABA as a way of sharing our collection of resources with others. As a former teacher, her passion is in using ABA in classrooms in order to create positive and comprehensive learning environments for all students. She is the Clinical Director at a private school in Toronto and is loving getting to make a difference in the lives of children and families daily. She is passionate about making the principles of ABA practical, doable and relevant to every child in any situation.
Shayna Gaunt, MA, R.B.A (Ont), BCBA is a dedicated professional in the field of Applied Behavior Analysis (ABA) and co-founder of How to ABA, an online resource and community supporting ABA professionals. With over two decades in the field, a Master’s Degree in ABA from the University of Nevada Reno, and extensive international experience, Shayna brings a vast expertise across diverse settings. She emphasizes collaborative excellence in direct therapy, supervision, and training, striving to deliver high-quality services and resources to clients and fellow ABA practitioners. Through How to ABA, Shayna aims to make ABA principles accessible and practical, fostering a community where professionals can share, learn, and grow together.




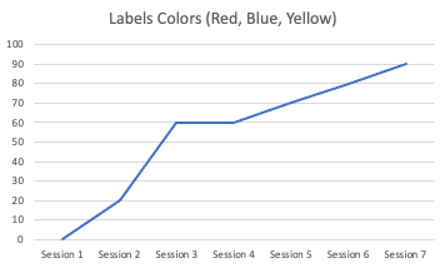 Figure 1. Graph with an increasing trend.
Figure 1. Graph with an increasing trend. Graph with a decreasing trend.
Graph with a decreasing trend.