With the start of Summer comes endless possibilities of fun in the sun, from beach days to festivals and fireworks. But for many children with sensory challenges, some of these activities can be overstimulating. Instead, there are many fun and individualizable activities for your child to enjoy which meet their sensory needs. Let’s review a few activities that you and your family can try before Fall comes back around.
Water Tables
Water tables make for a fun way to explore different textures. There are many activities you can do with water tables to make them both fun and educational.
Place objects in the water table and give your child a net to “fish” them out. You could use letters, numbers, colored ducks, etc.
Fill it with dirt and rocks and dig or drive through it with toy trucks.
Fill the table with water beads, sand, shaving cream, or pom poms and explore the different textures.
If your water table is small enough, you could place the water table in your bathtub. Your child can enjoy water play in a structured way indoors on rainy days.
Scavenger Hunts
Scavenger hunts can be so exciting. They encourage physical activity, exploring, and learning about the environment. They also require problem-solving and creativity. There are countless ways to make these unique and enjoyable.
Pick a theme of high interest for your child and curate the scavenger hunt around that theme. Examples: Dinosaurs, princesses, letters, etc.
Choose items to search for that your child is currently working on learning about. For example, if they’re working on identifying animals, the scavenger hunt may consist of animal toys, stuffed animals, animal puzzles, etc.
Take a walk around the neighborhood, searching for safety signs, items in nature, or other objects around your environment.
Obstacle Courses
For your highly active sensory seeker, obstacle courses are a unique way to burn energy and have fun. These may be used to work on balance, coordination, and motor planning as well. This is another great activity where creativity can shine.
Set up cones or other barriers to run or jump or hop around.
Place climbing blocks, stepping stones, or other uneven surfaces to walk on and climb through.
Move through the obstacle course like different animals-Bear crawl, hop like a bunny, etc.
Water Play
For children who enjoy water, but get overstimulated in large crowds like there are at waterparks or the beach, there are so many other fun ways to explore the water.
Sprinklers – The sprinkler level may need to be adjusted to fit your child’s comfort. For example, if your child does not like getting their face wet, but does like to run through the water, having the sprinkler level low would meet that desire.
Water balloons – While some children with hypersensitivity to stimuli may not enjoy a water balloon fight, they may find enjoyment in the actions of throwing water balloons and watching them splash when hit on surfaces.
Let them hose the car or bikes, fill up a bucket with water, or water the plants. So many options!
Fall is right around the corner. Before the cool air comes back around, try some of the activities suggested above to enjoy the weather in a sensory-friendly environment. Be sure to personalize each activity around your child’s interests, skillset, and needs.
About the Author
Ashleigh Evans, MS, is a Board Certified Behavior Analyst. She has been practicing in the behavior analysis field for over 13 years and opened her own independent practice in early 2022. Her experience has been vast across different age groups, diagnoses, and needs. She is passionate about improving the field through education, reformative action, and better supervisory practices, leading her to create content and resources for families and ABA professionals which can be found on her website, www.evansbehavioralservices.com/.
Originally posted on July 21, 2022 by Different Roads to Learning
Written by Ashleigh Evans, MS, BCBA. Reposted with permission from Dr. Anton Shcherbakov, BCBA, Co-founder of ThinkPsych
Behavior analysts and other professionals in the ABA field are tasked with the job of creating behavioral and skill acquisition goals for their learners. Choosing behaviors and skills to target can be challenging, with many considerations to make. One vital consideration when developing goals is to determine whether they are socially significant.
What is Social Significance in ABA?
Social significance refers to goals that are, first and foremost, important to the learner. If your learner can verbally communicate what’s important to them, this should take the highest priority. Some clinicians may not consider a learner’s goals due to their age or communication barriers. However, by monitoring for signs of assent, you can learn a great deal about what is important to the learner, even if they cannot verbally answer what goals they want to work on.
Beyond what’s important to the learner, social significance considers what goals are important to stakeholders and to society as a whole. Socially significant goals are behaviors and skills that will improve your learner’s overall quality of life and well-being. Goals should never be chosen simply for the convenience of others.
Considerations to Determine if a Behavior is Socially Significant
You may find yourself asking a number of questions when contemplating targeting a particular goal. Let’s review several considerations to make when evaluating whether to target a particular goal.
Is this behavior important to my learner?
As previously stated, this is the most important aspect of social significance. If the skill is something your learner is interested in or a behavior that they are motivated to modify, this would be considered a socially significant goal. Goals that are important to your learner should almost always be prioritized.
Will the skill cause harm or distress?
This may seem like an obvious one, but it’s important to carefully consider. Many ABA practices that were commonplace even just a few short years ago are now known to be potentially harmful, with advocates and autistic adults bringing concerns to light. For example, a lack of eye contact is common in people with autism. Some professionals consider eye contact to be an important social skill to target. However, many autistic individuals report adverse physiological reactions to eye contact. In other words, forcing eye contact may physically hurt. Research on this topic found that autistic adults and teens experience a wide range of reactions when engaged in eye contact including dizziness and headaches, increased heart rate, and nausea. Many also reported sensory overload when making eye contact, resulting in an inability to process and integrate visual and auditory information at the same time. Taking into consideration this information, one would likely determine that eye contact is not socially significant unless it is a skill the individual reports a desire to improve upon. When developing goals, determining whether targeting the skill may cause harm is vital.
Does the goal support the learner’s social-emotional development?
Social-emotional development is vital for a happy, healthy life. Research has found that a strong foundation of social-emotional skills can significantly improve a child’s future social, emotional, and academic success.
Social-emotional learning encompasses a wide range of skills related to self-awareness, self-control, social awareness, relationship skills, and responsible decision-making. Due to the social communication challenges that autistic children commonly experience, the development of these skills often takes more strategic planning and effort on the part of therapists, educators, and caregivers.
Make social-emotional learning enjoyable for your learner by engaging them in games and other preferred activities that support the development of these vital skills. Chat Chains, for example, is a unique game that targets developing conversational skills, teaches emotional awareness, and practices important social skills, all while having fun!
Will the skill enhance safety?
A staggering 28% of deaths of autistic people result from accidental injury. This includes causes such as suffocation, asphyxiation, and drowning. Of the general population, 6.5% of deaths result from accidental injury. This likely plays a significant role in the drastically reduced life span. The average age of an autistic individual at death is about half that of the general population, 36 years of age.
While these statistics are bleak, they highlight the need for a focus on skills that will keep your learner safe. Following crucial safety instructions, navigating situations such as getting lost, communicating personal information, identifying hot and poisonous items, and water safety are all socially significant skills that can keep your learner safe.
Will the skill increase independence?
Promoting independence can build self-esteem, increase the generalization of skills across environments, and improve your learner’s overall satisfaction in their life. There are countless socially significant skills that can promote independence. Teaching communication and self-advocacy skills are arguably the most important skills necessary for enhancing independence. Self-help skills, money management, household chores, and vocational skills are also important to consider when developing goals that will increase your learner’s independence.
Has the child acquired the necessary prerequisite skills?
Oftentimes, caregivers and professionals have big goals for their children or clients. This might result in jumping the gun a bit in implementing big-picture goals such as toilet training. However, it’s important to consider whether the child has developed the necessary prerequisite skills before targeting a goal. A simple example of this is following multiple-step instructions. Perhaps a parent asks you to target instructions such as putting away their shoes and backpack when they arrive home. While these may be socially significant goals, if the child cannot yet follow simple single-step instructions, then it would not be appropriate to target multiple-step instructions.
Final Words
Developing socially significant goals for your learners takes time and consideration. Ensuring that the goal will improve the learner’s quality of life and well-being should always be at the forefront.
About the Author
Ashleigh Evans, MS, is a Board Certified Behavior Analyst. She has been practicing in the behavior analysis field for over 13 years and opened her own independent practice in early 2022. Her experience has been vast across different age groups, diagnoses, and needs. She is passionate about improving the field through education, reformative action, and better supervisory practices, leading her to create content and resources for families and ABA professionals which can be found on her website, www.evansbehavioralservices.com/.
About ThinkPsych and Dr. Anton Shcherbakov
ThinkPsych is a company committed to making fun and evidence-based toys for social emotional learning. Co-founder Dr. Anton Shcherbakov is a licensed psychologist and board certified behavior analyst. He has co-authored peer-reviewed research on topics that include depression and suicide prevention. He is also a nationally recognized expert and frequent presenter at national conferences on the treatment of anxiety, ADHD, autism spectrum, OCD, and related conditions. He previously taught at the Rutgers Graduate School of Applied and Professional Psychology. In addition to his work at ThinkPsych, he provides psychotherapy to children, adolescents, and adults at The Center for Emotional Health of Greater Philadelphia. In his free time, he enjoys traveling with his family, cooking meals with too many ingredients, and watching the latest Netflix documentary series.
By Dr. Stephanny Freeman and Kristen Hayashida, BCBA
Super Parents! We know you used your Executive Function (EF) powers to prepare for summer! For most of us, this process started as early as February with camp sign-ups, enrichment programs, juggling schedules and the time-off of others, extended family, competing obligations, and maybe even a family vacation. We see summer as a hot/humid gigantic puzzle of weeks that must be filled with fortifying activities that surely and absolutely develop our young children’s minds, bodies, and souls! We fear expense, we fear boredom, we fear regression, we fear pushback or dislike, ARGH!!!
But truthfully, for us, as summer approaches, we just feel accomplished if we found anything where the kids would at least come home ‘happy and exhausted!’
That said, we know the LAST thing you want to think about is adding more pressure to yourself on how to better “enrich” your child’s summer.
Hold on though… what if we said it was easy, part of what you already do, and would embed into your summer plans?
Pass on your EF super-powers and turn any activity into executive function practice that will not only enhance and develop your child’s skills but may actually make your life easier!
Planning
The easiest and most obvious is Planning. Planning entails the ability to identify all the different steps needed to achieve a specific goal and in what order those steps need to happen. Involving your children in the planning of any outing, particularly road trips or vacations is an incredible way to develop their EF skills. For example, for very young children, have them download and print pictures of different sights, people, or locations that you might see on the outing/trip.
Organization
Organization includes the capacity to prioritize and make decisions about which tasks to undertake, as well as anticipate and keep track of needed materials or resources. So, use the printed pictures and put them in order using a calendar and a map to take into account location/day/participants. Then make a list of “things you’ll need” for each event. For example, if you are going swimming, make a list of the items needed for the pool. It is not lost on us that you all do this anyway but we encourage a little extra time to include your kids and have the visuals. We’ll bet it will also improve the likelihood that you’ll have everything you need!
Time Awareness
Time Awareness is part of the broader skill of time management which includes the ability to anticipate how long tasks might take and be aware of time constraints. This is developmentally challenging for younger children who are still emerging in their understanding of the abstract concept of time; however, you can still enhance experiences and continue development within something you are already doing. A great opportunity for helping children develop time awareness is at amusement parks, fairs, or zoos. Look at showtimes for when the animals are being fed and help your child consider how long they have to see other exhibits before the show. Use a map and have your child consider how long it will take to walk from exhibit to exhibit and ask their input for when might be best to stop for lunch. Using a combination of visuals (e.g., maps, showtimes) and verbal support, you can help your child think about time in a more tangible way.
Inhibitory Control and Problem Solving
Within plans, there are always smaller activities. For example, a beach day might include building sandcastles, going boogie boarding, and splashing in the waves. You and your child have planned the outing, organized what you need to bring, and timed out the outing so you can squeeze all the activities in. Once at the beach, Inhibitory Control and Problem Solving become your new EF goals! Inhibitory Control involves the ability to regulate one’s attention, behavior, thinking, and emotion. We are hard-wired to be aware of and prime our children for what is unsafe (stay close to our spot on the beach, no going into the water without us, etc.). But what about doing some priming for emotion? For example, have your children try to identify what things might go a different way than expected and then come up with potential solutions. It doesn’t have to be doom and gloom (i.e., what might go wrong), but more fun and exciting – like a challenge. Ask your child as they are building their castle… “What will you do if a huge tsunami comes to your world?” Praise them for their control and problem solving and use that same language when other unexpected things happen (e.g., the Godzilla neighboring child that inadvertently stomps through the castle).
Cognitive Flexibility
Summer is also a great time to encourage cognitive flexibility. This entails having your child shift their thinking! Change their approach! Recognize and accept when something needs to be changed. There should be a sign that parents carry with them over the summer because in my experience, everything summer-related required a relaxed attitude to keep my sanity. Not kidding — carry a sign that says, “Bendy is Fun!” and remind the children of this fact any time you use pliable materials in play (e.g., sand, play dough, clay, craft materials). These materials are fun because they can be used in so many different ways and be remolded into something else. During summer activities, point out constantly to your children with the “Bendy is Fun” board that when you tried something new, or did something different, it was being “bendy” and worked out for the best.
EF skills are very intertwined and build upon each other. We often call them “cogs” in our brain machine. EF strategies often overlap and facilitate one another so you can do just a few tiny little changes to your summer activities and make them really enriching to benefit EF skills. EF skills are for life and learning. Starting your children early and practicing these skills in the most embedded and easy ways will ensure that your summer is filled with enrichment!
About the Authors
Dr. Stephanny Freeman is a clinical professor at UCLA, a licensed clinical psychologist, and Co-Directs the Early Childhood Partial Hospitalization Program (ECPHP). For 20 years, she has educated children with ASD and other exceptionalities as a teacher, studied interventions for social emotional development, and designed curriculum and behavior plans in school and clinic settings.
Kristen Hayashida is a Board Certified Behavior Analyst at the UCLA Early Childhood Partial Hospitalization Program (ECPHP). For the last 10 years she has served as a therapist, researcher and educator of children and families living with autism spectrum disorder through the treatment of problem behavior.
This month’s ASAT feature comes to us from Dr. Karen Parenti, MS, PsyD CEO/Executive Director, and Heather Rothman, BS, LBS, Director of Day Services, Special Friends Foundation. To learn more about ASAT, please visit their website at www.asatonline.org. You can also sign up for ASAT’s free newsletter, Science in Autism Treatment, and like them on Facebook!
I am the parent of an adult with autism, who will soon transition from a school program to adulthood. I am reading about engagement as an indicator of good programming. What does it mean and how can I tell if a program promotes it?
Answered by Karen Parenti, MS, PsyD, CEO/Executive Director, andHeather Rothman, BS, LBS, Director of Day Services, Special Friends Foundation
Transition into adult programming is an important, but often stressful, process for families and individuals to experience. Adult programming should be designed to build skills and to promote happiness. Essentially every parent wants their adult child to have a high quality of life, to be offered activities they find enjoyable, and to be self-determining. For this to happen, the individual needs to be fully engaged in the program. Family members, clinicians, behavior analysts, program specialists, administrators, and social workers who provide services to individuals with intellectual and developmental disabilities and autism (ID/A) need to remember the importance of active engagement when planning and implementing programs as well as when designing goals.
Imagine for a minute the perspective of an individual receiving services. In most cases, this means the individual has had a diagnosis of some kind since childhood. The current model for treatment in children may result in a consistent feeling of “other-ness,” whether that looks like segregated classrooms, peer mentors, wraparound therapists, or specialized activities dependent on the label. From the perspective of the individual, this can look like endless task demands, shallow or contrived social interactions, decreased opportunities for genuine relationships, and severely limited access to the community. In addition, for a lot of the individuals served, the ability to protest “appropriately” is diminished, either because of communication barriers or skill deficits, or because they are not given opportunities to practice these skills. Empowering individuals to become architects of their experience and to express dissent and discomfort are crucial goals to ensure agency, assent, and quality of life. In addition, providing more choices can be part of a trauma-informed focus of care, and can ensure that individuals are served in a humane and compassionate manner (Rajaraman, 2021).
Although engagement as a clinical construct has yet to be deeply researched in applied behavior analysis (ABA), there has always been an ongoing interest in social validity, which is an emerging interest in the field (Morris et al, 2021). It should be noted that in the workforce, engagement has been defined for employees and became understood as a configuration of vigor, dedication, and absorption that motivates exceptional work performance (Leiter, 2019). Engagement, just like all metrics of success in the human services and special education fields, is personal and individualized for everyone. It is therefore important that engagement is individually assessed and monitored for everyone; from a parental or caregiver perspective, it is important to help the team understand how your family member expresses happiness, dissatisfaction, and protest. Teams may work to ensure high levels of satisfaction by ensuring that individuals attend the program regularly (or determine why there might be issues with attendance), and that preferences are identified in goals addressing the social, work, and living environments. It is imperative that teams ask themselves important questions such as is assent gained, routinely assessed, and honored? Moreover, does the individual seem happy while in the adult setting?
In recent years, the focus on engagement has altered the way in which quality programs are identified. Historically, there was a common focus on productivity and on compliance. While productivity remains relevant, engagement can become a main focus of intervention. In addition, the quality of interactions with individuals is also highly valued. Providers should focus on engaging the individual first by developing a positive relationship and pairing themselves with reinforcement. Individuals served, like all people, will always respond to genuine respect and regard, and this should be a foundation of service provision.
This value on engagement is consistent with heightened awareness in the field of ABA to ensure that all intervention is humane and compassionate, and that self-determinism is maximized for all individuals. In the context of adult intervention, such qualities can be seen in the extent to which engagement is observable. Some questions can be asked, and some behaviors associated with engagement can be observed.
Engagement is observable when a person is enthusiastically participating in their program. Choice has emerged as a necessary piece of engagement; individuals should be offered a range of meaningful activities from which to select, while still retaining the right to refuse. This is closely related to the Positive Approaches paradigm defined by Guy Legare (2002), who “encourages us to see clearly and honestly the good reasons and adaptive qualities of even the most troubling behavior, no matter whose behavior it is.” Provider agency staff and special education school personnel who excel at this skill set seem to be the ones to whom an individual is a person first, and these professionals never see an individual as a “case” or “set of behaviors.”
Although clinicians have considerable access to different types of preference assessments, as well as training on how to use them, it’s valuable to keep in mind all the factors that influence the efficacy of reinforcers with regards to engagement. For example, an individual may be more likely to be engaged in an activity in which they are participating with others, in a novel location. Engagement is a reinforcer unto itself but requires a deep knowledge of the individual and their preferences as well as focusing on the relationship between the individual and the staff member. As with any other treatment focus, engagement depends heavily on a positive, nurturing, and entertaining relationship between two people.
Engagement has to be individualized so that it can be maximized. It is observable, able to be defined and measured, and important to consider in placement, goal development, and in the ongoing assessment of progress. Programs can follow some general guidelines to increase the likelihood of enthusiastic participation, build active engagement, and foster self-determinism. These concepts include but are not limited to:
Demonstrating unconditional positive regard – Staff and clinicians need to ensure that the individual they are working with is always treated with respect and dignity. Building rapport with each individual and communicating with those individuals regularly is essential to creating a compassionate, humane treatment environment.
Attain Assent – Assent is emphasized in the Ethics Code (BACB, 2022), and should be secured whenever possible. Recent research indicates that this is an area that can improve and can also be done with individuals who are non-vocal (Morris, 2021). The team should ensure that the individual is continually involved in making choices regarding their daily activities. Attain assent for activities, and regularly check in about whether the individual is still willing to do the tasks. Honor withdrawal of assent.
Solicit and accept feedback – Being receptive to feedback means allowing individuals to critique and course-correct staff behavior. Although feedback can be directly solicited, individuals provide feedback in lots of indirect ways as well. It is important to ensure there is reciprocal shaping of interactions between staff and individuals. Being open to changing the approach, based on cues from the individual, allows for the individuals served to have a measure of control over their own treatment, which increases the likelihood they will be enthusiastic participants, and therefore engaged.
Prioritize needs – Staff and clinicians need to ensure that the individual they are working with has their basic needs always met.
Respect all forms of communication – Staff and clinicians need to respect all verbal and nonverbal communication from that individual. These subtleties can be missed if the staff is not paying close enough attention. It’s important to remember that challenging behaviors are often an important form of communication.
Create a supportive environment – An environment where the individual is supported and connected is one where they will be actively engaged, will thrive, will learn, and will master skills and increase competencies. Individuals can get discouraged easily and can become disengaged. In these situations, a little support or assistance can go a long way. Other considerations for a supportive environment could include instruction and activities in novel locations, with persons that are preferred by the individual, and by attending to the individual’s preferences to the maximum extent possible.
Create Novelty – As stated earlier, novelty also helps increase engagement. When educators introduce something new, they provide opportunities for learning skills with a new item. In many cases, exploring a new item (or scenario, song, story, etc.) creates new opportunities for thinking, for understanding how things work, or connecting existing concepts in a new way. Novelty can also allow staff to engage the individual in a new way.
Be willing to share control of the instructional context – Clinicians or staff can ensure that choices are presented as often as possible. There is always a choice to be offered. For example, instead of saying “now it’s time to get dressed”, a staff can say, “Would you rather put on your shirt or your socks first?” It’s also important to find a way to say “Yes” to a request as often as possible. If an individual is asking for something that is unavailable, instead of saying “No,” staff can offer a different time when the item/activity is available. It is important to be as specific as possible.
In summary, if a provider, agency, or special education school wants to increase active engagement while being genuinely helpful, staff and clinicians should partner with the individuals and their team members in selecting goals, developing instructional procedures, and identifying meaningful outcomes. This is the essence of social validity and is essential to compassionate care.
Legare, G. (2002). Positive approaches as a paradigm. In Positive approaches: Identifying mental illness in people with developmental disabilities, (2nd Ed.) OMR Statewide Training and Technical Assistance Initiative.
Morris, C., Detrick, J. J., & Peterson, S. M. (2021). Participant assent in behavior analytic research: Considerations for participants with autism and developmental disabilities. Journal of Applied Behavior Analysis, 54(4), 1300-1316. doi: 10.1002/jaba.859.
Rajaraman, A., Austin, J., Gover, H., Cammilleri, A., Donnelly, D., & Hanley, G. (2021). Toward trauma‐informed applications of behavior analysis. Journal of Applied Behavior Analysis, 55(1), 40-61. 10.1002/jaba.881
Schramm, R. (2011). Motivation and reinforcement: Turning the tables on autism. Pro-ABA.
Parenti, K., & Rothman, H. (2023). What is the importance of engagement when working with individuals with intellectual and developmental disabilities and autism? Science in Autism Treatment, 20(01).
About the Authors
Dr. Karen Parenti works as the CEO/Executive Director of Special Friends Foundation. She has extensive experience in ABA and in developing and overseeing group homes, day services, and rehabilitative programs for individuals with intellectual and developmental disabilities and autism. She also serves as the treasurer of the MAX association’s board where she continues to advocate for the needs of the individuals she serves. Karen earned her Bachelor’s degree in psychology from York College of PA, her Master’s Degree in Human Services Administration from Springfield College in Wilmington, DE and her Doctorate Degree in Clinical Psychology from Immaculata University.
Heather Rothman works as the Director of Day Services for the Special Friends Foundation. She has worked with individuals with disabilities in a variety of settings and roles for over twenty years. Heather is committed to helping individuals with disabilities and Autism access choices, connect with their communities, and design the life they want. She is a Licensed Behavior Specialist with extensive experience with behavior support services in early intervention, school-aged, and adult populations. She designed and built a school-to-work transition program that won an international award for Variety-The Children’s Charity. She has taught at Penn State, developed trainings for the Public Health Management Corporation, and worked with Merrill Lynch on accessibility and community inclusion programs. She is passionate about universal accessibility and designing programs that create strong communities. Heather has her Bachelors of Arts in Organizational Management from Ashford University and a Master’s Degree in Applied Behavior Analysis from Saint Joseph’s University.
I was first introduced to the idea of prompting and fading when I co-ordinated a home based early learning program for my eldest son, Christopher, who is on the autism spectrum. I soon came to appreciate how important these strategies were and are in supporting his learning. We are now into his teenage years and whilst the skills he is learning are far more complex compared with those early years, the use and importance of prompting and fading remains unchanged.
About prompting
A prompt is a cue (or hint) given to a student to encourage them to learn a new skill. There is extensive evidenceto support my own experience that prompting is a highly effective way of teaching. An example of this evidence is noted at the end of this article.
Flashcards and prompting
A lot of the work we did around prompting with Christopher in the early years of his life related to the use of flashcards. We used them to expand his vocabulary, articulate words clearly and put together sentences. We also used them to build his academic skills in literacy and numeracy and his capacity for problem solving.
The different types of prompts
There are five different types of prompts and we used all of them in our flashcard based activities. These prompts are ranked accordingly to the level of support they offer, with 1 being the most supportive and five the least.
Full physical Example: I placed my hand over Christopher’s hand and guided him to place the flashcard he was holding over the associated one on the table – so the image of the sock was placed on top of the shoe, rather than on the image of the bed or the bowl
Partial physical Example: I gently touched Christopher’s shoulder – to indicate it was time for him to respond to my request of naming the flashcard I was showing him.
Modelling Example: I sorted the flashcards on the table into groups – animal, transport and instrument. I then shuffled the cards and asked Christopher to sort them in the same way
Gestural Example: I nodded as he started to place the letter A next to the image of the apple. It provided him with the encouragement and confidence to continue with B and C.
Positional Example: I placed two associated cards on the table next to one another so that Christopher could connect the two – so the picture of the fork was next to the picture of the person eating and the picture of the bed was next to the picture of the person sleeping
The goal is to select the type of prompt that is the least intrusive and results in the student providing the correct response. So, if a modelling prompt is not working then a partial or full physical prompt should be tried.
Why prompts need to be faded
Whilst prompts are a great teaching strategy, it is equally important that they be faded over time. You might ask why. The answer is so that the student doesn’t become dependent on the prompt. We were mindful of this in Christopher’s early learning program. There were instances where we started with a full hand over hand prompt. We then faded to a gestural prompt (by pointing at the flashcard) before omitting the prompt all together.
I like to think of prompting and fading as stepping stones on the way to independence with a new skill. Christopher and I have trod on those stones for a number of years now and going forward I know there will be more. I hope there will be more, As I’m so appreciative of the opportunities for learning they ultimately afford my son.
Citations
1 Hayes, D., (2013) The Use of Prompting as an Evidence Based Strategy to Support children with ASD in School Settings in New Zealand. ERIC 1-5
About The Author
Kate is the owner of Picture My Picture, an international business which specializes in educational flashcards. She is the mother of three boys, Christopher, Louis and Tom. Christopher is on the spectrum of Autism. The flashcard based teaching program she oversaw in the early years of his life was the inspiration for the business she owns today.
This article was originally posted on November 17, 2021 by Different Roads to Learning.
by James T. Ellis, Ph.D., BCBA-D and Christine Almeida, Ms.Ed., Ed.S., BCBA
Since first publishing Socially Savvy, there has been so much progress in the way that we approach, assess, and support students with learning differences. Because we are not only the writers of Socially Savvy, but also users of it, we have also learned so much over the past decade as we have used the assessment and intervention strategies with the children that we have supported. Our belief that there is not a “one size fits all” approach has strengthened. The social skills that we identified in Socially Savvy as important for young children are skills that might be important for some children in some settings, may not be important for other children, and there may be other skills that we have not identified that might be important for other children. We continue to want to make sure that Socially Savvy is used as a guide to help therapists, educators, and parents determine what skills are important to target for the children who they are supporting.
Being a good educator requires us to grow and learn along with the children that we teach. That is why we have released the Socially Savvy Assessment Protocol with Extended Objectives. In addition to adding a second objective for each skill, we have also freshened up some of the initial objectives. A greater understanding of neurodiversity has developed over the past decade, and we want to make sure that we are carefully considering that when we are making decisions about what social behaviors to target for change, which behaviors to accommodate through environmental changes, and which behaviors to embrace and encourage from children. Part of our reason for updating the objectives is to make sure that we are being conscientious about the diverse ways that children act, think, learn, respond to sensory input, and process the world around them.
Additionally, we have realized that it is helpful to have more objectives for the skills that are part of the Socially Savvy Checklist because children are working on objectives in multiple settings and need to apply the skills in a variety of environments – school, home, community, clinic, etc. What might be an appropriate objective in one setting may not fit the environmental expectations of another setting. We have provided an additional objective for each targeted skill, in the hope that one of the objectives might be a fit for the child with whom you are working, or that the objectives might provide inspiration for developing an objective that matches the needs and environment of the child.
Being a good educator requires us to be creative in how we teach and motivate children to learn. This is especially true when we are teaching social skills, which are complex and often difficult to break down into steps that are achievable for the child and manageable for staff to teach. We want children to learn in a way that is fun, exciting, and continues their growth and curiosity. We also want staff to have fun while they are teaching. By providing an additional objective, we are trying to spark that creativity and help educators make teaching the targeted skills more fun, both for the child and for the teacher. If the objective is clear to staff, appropriate for the setting, and taught in a more fun way, staff are going to work on that skill more. The more targeted social skills can be embedded in simple games and throughout the natural environment, the more fun it should be for staff to run. Consequently, the child is going to have more teaching opportunities embedded in a fun context and is hopefully going to learn more quickly. This then has the added benefit of staff being reinforced by seeing the child learn at a faster rate. If we are having fun, it’s easier for staff to teach and the child to learn!
We also acknowledge and recognize that educators and professionals supporting the social growth of children, whether in a school setting, a family’s home, the community, or a clinic are busy and often overwhelmed. We hope that refining and adding to the objectives will make your work a bit easier. We respect the great work that you all do in helping children grow to their fullest potential. As always, we appreciate hearing from all Socially Savvy users, whether parents, special educators, behavior analysts, or other professionals. Your thoughts and comments have been invaluable. The idea that you find the curriculum useful has been humbling.
About the Authors
James T. Ellis, PhD, BCBA-D earned his PhD in Clinical Psychology from West Virginia University and is a licensed psychologist and board certified behavior analyst. For over 20 years, Dr. Ellis has provided services for children with autism spectrum disorders and their families. In 2008, he helped found the Step by Step School for Children with Autism in Guyana, South America and in 2012, he founded Step by Step Behavioral Solutions, through which he continues to provide consultation and therapeutic support to individuals with autism spectrum disorders and their families.
Christine Almeida, MSEd, EdS, BCBA earned her MSEd in Special Education and EdS in Behavioral Education from Simmons College in Boston, MA. Ms. Almeida is a practicing board certified behavior analyst in the Boston area who has worked in both private and public schools. She currently provides oversight of services for young children with autism spectrum disorders for a public school. Ms. Almeida has presented workshops at the local, regional, and national levels on the subjects of educational assessment, play intervention, and social skills.
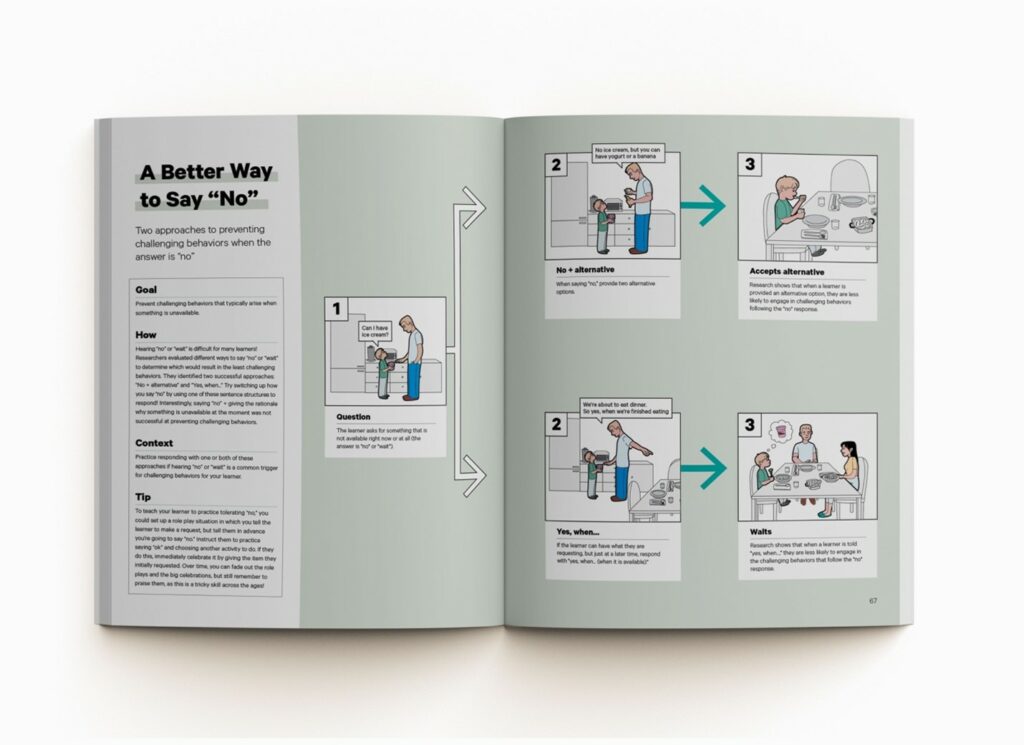
By Morgan van Diepen, M.Ed., BCBA, Co-owner of ABA Visualized
Hearing “no” or “wait” can be challenging for kids of all ages! In fact, as a BCBA, this is one of the most common requests for support that I hear from families. Luckily, researchers have tested out three ways to say “no” when something is unavailable, and the results show how slightly changing our response can actually prevent challenging behaviors! Let’s look at the scenario of a child asking to play a computer game, but the parent is currently using it for work. Which of the three methods do you think was the most effective?
“No” + Explanation. In this common approach, the parent says it’s not available and gives the honest reasoning: “Not right now. I’m working on the computer.”
“No” + Explanation + Alternative. Now, we’ve added an extra suggestion of something that is available: “Not right now. I’m working on the computer, but you can play basketball outside with your brother.”
“Yes” + Contingency. Here, even though our answer is “no,” we’re actually saying “yes!” This can be described as a “yes, when…” statement, where you are describing when the requested item or activity will be available: “Yes, you can use the computer when I’m finished with this meeting at 2:00.” It can also be used to set expectations of what they need to accomplish before the request is available: “Yes, you can use the computer when you finish your homework.”
So, which do you think resulted in the fewest challenging behaviors?
In this research study, the 2nd and 3rd approaches were equally successful at almost completely preventing vocal protests, aggression, and threats! By just changing the way we say “no,” we can help our learners accept this answer more easily. Little changes that create big results! Strategies like these are perfect for parent training sessions during ABA. Here’s a template parent training goal you could use with families who would like more support in this area:
When (client name) requests for something that is unavailable (provide examples specific to the client), parents will either respond with “No” + Explanation + Alternative (provide example specific to the client) or with “Yes” + Contingency (provide example specific to the client) in attempts to prevent challenging behaviors relating to tolerating “no,” in at least 80% of opportunities across 2 consecutive weeks.
Looking for a more engaging way to lead parent training sessions and teach effective strategies like this one? Check out our 2nd edition ABA Visualized Guidebook, where we’ve visualized 27 evidence-based strategies (including this one!) as step-by-step illustrations, making behavior strategies easy!
Article reference: Mace, F. C., Pratt, J. L., Prager, K. L., & Pritchard, D. (2011). An evaluation of three methods of saying “no” to avoid an escalating response class hierarchy. Journal of applied behavior analysis, 44(1), 83–94.
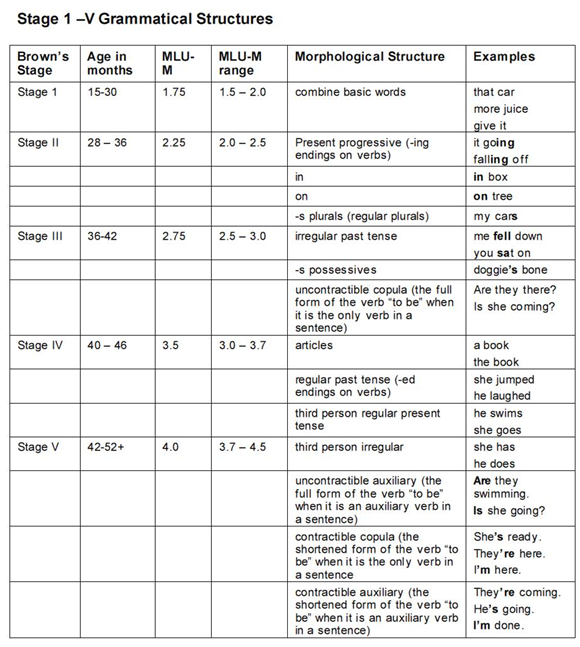
Teaching language skills is one of the most frequent needs for children with autism, but also one of the most misunderstood skillsets amongst both parents and practitioners. The desire to hear your learner speak in full sentences can be overwhelming, making it especially difficult to take a step back and consider what it means to communicate and how communication skills develop in neurotypical children. Many times we get hung up on what a child should be capable of communicating at a certain age, rather than focusing on what they are capable of communicating at this stage of development.
Many practitioners and curricula utilize Brown’s Stages of Language Development.* Brown described the first five stages of language development in terms of the child’s “mean length of utterance” (or MLU) as well as the structure of their utterances.
Sometimes it is necessary to compare a child to his or her same-age peers in order to receive services or measure progress, but it can be detrimental to focus on what a child should be doing at a specific age instead of supporting them and reinforcing them for progress within their current stage.
Research has suggested that teaching beyond the child’s current stage results in errors, lack of comprehension, and difficulty with retention. Here are some common errors you may have witnessed:
The child learns the phrase “I want _____ please.” This phrase is fine for “I want juice, please” or “I want Brobee, please,” but it loses meaning when overgeneralized to “I want jump, please” or “I want play, please.” It’s better to allow your learner to acquire hundreds of 1-2 word mands (or requests) before expecting them to speak in simple noun+verb mands.
The child learns to imitate only when the word “say” is used. Then the child makes statements such as “say how are you today,” as a greeting or “say I’m sorry,” when they bump into someone accidentally. Here, the child clearly has some understanding of when the phrases should be used without understanding the meanings of the individual words within each phrase.
The child learns easily overgeneralized words such as “more.” This is useful at times, but the child can start using it for everything. Instead of saying “cookie” he’ll say “more.” Instead of saying “train,” he’ll say “more.” And he may say “more” when the desired item is not present, leaving the caregiver frustrated as he/she tries to guess what the child is requesting. Moreover, as language begins to develop, he may misuse it by saying things such as “more up, please.”
The child learns to say “Hello, how are you today?” upon seeing a person entering a room. A child comes into the classroom and the learner looks up, says “Hello, how are you today?” The child responds, “Great! Look at the cool sticker I got!” Your learner then doesn’t respond at all, or may say “fine,” as he has practiced conversations of greeting.
These are only a few of the common language errors you may see. While you may want your learner to speak in longer sentences, your goal should be to have them communicate effectively. With this goal in mind, it becomes essential to support them at their current stage, which means it’s essential to assess them and understand how to help them make progress.
This is why I always use the VB-MAPP to assess each child and make decisions about language instruction. I need to have a full understanding of how the learner is using language, and then move them through each stage in a clear progression. I may want the child to say “Hello, how are you today?” But when I teach them that, do they understand those individual words? Do they comprehend what today means as opposed to yesterday or tomorrow? Do they generalize the use of “how” to other questions?
As you make treatment decisions for your learner, think about their current stage and talk about how to support your child with both a Speech Language Pathologist and an ABA therapist.
*Brown, R. (1973). A first language: The early stages. London: George Allen & Unwin Ltd.
About the Author
Sam is an ABA provider for school-aged students in Brooklyn, New York. Working in education for over 15 years with students with Autism Spectrum Disorders and other developmental delays, Sam utilizes strategies for achieving a multitude of academic, behavior, and social goals. She is also an assistant professor in the ABA program at The Sage Colleges and the Senior Clinical Strategist at Encore Support Services.
Originally published by Different Roads to Learning on July 10, 2014.
Token economies are structured reinforcement systems used with people across many different populations. They can be particularly useful for reinforcing behaviors and skills in children with autism and other neurodevelopmental differences.
A token economy works similarly to our world economy. A child earns tokens for demonstrating various skills and behaviors, which can then be cashed in for preferred items or activities. Token economies have a significant degree of individualization, making them highly effective at modifying behaviors.
Getting Started
Let’s consider the following tips for using token economies with children with autism.
Focus on one or two skills or behaviors at first
Well-meaning therapists, teachers, and caregivers might create a token economy with several different behaviors targeted. However, when introducing a token economy, you should start with only 1-2 behaviors or skills. This is necessary to help your learner associate earning tokens with specified behaviors. If they receive tokens for many different behaviors throughout the day, it may be more difficult for them to grasp why they are receiving the tokens. To help them make this association, identify the behaviors that are of the highest priority and start with those. As the learner advances and makes progress with their current goals, you can begin incorporating additional behaviors into the token economy.
Individualize the tokens
Tokens can be anything–tallies, stars, poker chips, stickers, or coins, for example. Individualizing the tokens to something the child enjoys can add an extra layer of reinforcement. For example, if you’re using a token board, you might use stickers of objects or characters that your learner enjoys such as vehicles, animals, or cartoon characters. You don’t want your learner to get distracted by and fixated on the tokens either though, so it’s important to consider that when choosing tokens.
Start with continuous reinforcement
Every aspect of your token economy should be individualized, however, it is often most beneficial to start a token economy with continuous reinforcement, then fade to intermittent. This is especially true for children with more limited language skills. As they begin to pair the behavior with the token, you can shift to providing tokens on an intermittent schedule, depending on an assessment of their unique needs.
Provide immediate reinforcement
Reinforcement should immediately follow the target behavior. When the learner demonstrates the target behavior, immediately provide the token and pair it with social praise. Praise should be behavior-specific, labeling exactly what they did to earn the token.
Don’t forget your backup reinforcers!
This one might seem obvious, but backup reinforcers are a common missing piece of token economies. Children may earn tokens throughout the day or week, with no plan built in for cashing them in for something else. Earning the tokens is only one part of a token economy. Make sure prior to implementation that you have a back-up reinforcer menu ready to go, with plans outlined for how many tokens are needed for each item or activity. Incorporate your learner into the planning of this to ensure the backup reinforcers are motivating to them.
Avoid token economies for behaviors that the learner is already motivated to complete
There is much concern and debate on whether token economies and external rewards in general reduce intrinsic motivation. Research has found that external rewards actually increase intrinsic motivation, but only when the person was not already intrinsically motivated to engage in the behavior (LeBlanc, 2004). For example, imagine a child who enjoys sweeping the floor. She willingly sweeps every day, without external reinforcement. Her mother decides to begin paying her for completing this chore. Adding external rewards to a task that she was previously intrinsically motivated by could actually decrease her intrinsic motivation to complete that task. However, if the same child is not intrinsically motivated to brush her teeth, adding external rewards can increase her intrinsic motivation to brush her teeth. Therefore, only target behaviors that the child is not already motivated to engage in.
Monitor success and adjust
Token economies should be continuously evaluated. Monitor your learner’s progress and make adjustments when necessary to ensure continued progress through their personalized goals. With a well-planned and executed token economy, your learner can make socially significant gains in skills and behaviors.
References
Dalphonse, A. (2022, October 12). Token economy: Examples and applications in Aba. Master ABA. Retrieved May 1st, 2023, from https://masteraba.com/token-economy-2/
Kazdin A. E. (1982). The token economy: a decade later. Journal of applied behavior analysis, 15(3), 431–445. https://doi.org/10.1901/jaba.1982.15-431
LeBlanc, G., 2004. Enhancing Intrinsic Motivation Through The Use of a Token Economy.
About the Author
Ashleigh Evans, MS, is a Board Certified Behavior Analyst. She has been practicing in the behavior analysis field for over 13 years and opened her own independent practice in early 2022. Her experience has been vast across different age groups, diagnoses, and needs. She is passionate about improving the field through education, reformative action, and better supervisory practices, leading her to create content and resources for families and ABA professionals which can be found on her website, www.evansbehavioralservices.com/.
Take a look inside the newest book from Autism Partnership. Reprinted with permission from the authors.
Foreward
By Dr. Ron Leaf
I was sure that Clinical Judgement would be my last book. It was intended to help the new generation of behaviorists learn about some of ABA’s pioneers that seemed to have been forgotten. Those that inspired us. How could I “retire” without people knowing about Joseph Wolpe, Sandra Harris and Don Baer? Recently, however, it became painfully clear that there is another area that has been sadly neglected.
Social media has been abuzz about a new movement: “compassionate behaviorism.” I was perplexed! First, this group of social media bullies were discussing “compassion.” Moreover, this small group of practitioners was acting as if old concepts such as “therapeutic alliance” and being “curious listeners” were new. They seemed unaware that Carl Rodgers discussed this in 1957 and, in 1999, Richard Fox shared his deep concern that behaviorists seemed to be neglecting the crucial need for becoming “behavioral artists.”
If the agenda was to rekindle this neglected area, I would have been thrilled. But it seems there is far more to their movement and that their agenda is creating tremendous collateral damage. For example, they argue that true “compassionate behaviorists” should not give corrective, or sometimes even positive, feedback. In their view, all feedback is coercion. Of course, when providing corrective feedback, one should be sensitive and thoughtful. But to avoid corrective feedback completely is absurd, and ironically, not compassionate. I wouldn’t be an effective baseball coach if I didn’t tell a baseball player that he needs to track the pitch and stop pulling his head. I wouldn’t be an effective teacher if I didn’t provide corrective feedback regarding class presentations. And I wouldn’t be a good partner if I resisted listening to my wife’s feedback.
These practitioners also suggest that behaviorists should completely acquiesce to the agenda of their clients. That is, only work on those issues that the clients feel are important to work on. Obviously, we need to carefully listen to our clients, but often it is necessary to help our clients understand that only focusing on their top priority is not in their best interests. For example, a client may want to fix a toxic relationship, even when it’s not possible and clearly not in their best interest. Or, a client may want you to help them convince their partner that it’s okay for them to continue with their heavy drinking! Or that it’s preferable for them not to have friends, even though the research shows this can lead to isolation, depression, suicidal ideation and suicide.
Perhaps the most disturbing aspect of this movement is that these “compassionate behaviorists” are providing guidance on how to treat trauma. In order to treat trauma, one must have extensive education, training and testing to ensure that one has the necessary skill set. Otherwise, treating someone with depression or post-traumatic stress disorder can lead to catastrophic consequences. Essentially, they are encouraging folks to practice psychology without a license which is not only a misdemeanor in many States, but it is extremely dangerous!
For me and my colleagues, it was imperative to write The Clinician’s Toolbox: Rediscovering Compassionate ABA, not only to set the record straight about behaviorist history, but to learn from the clinical pioneers, and most importantly, to share the skills necessary to become effective behaviorists. Our goal is to inspire the new generation of behaviorists to receive the necessary education and training so they can truly become talented clinicians. Our ultimate hope is for the leaders in the field of Applied Behavior Analysis to understand that clinical training must become part of educational curricula, credentialling task lists and testing. Otherwise, we are not being “compassionate behaviorists”!
About the Book
Compassion is the cornerstone of effective ABA therapy, especially for patients with autism spectrum disorder. Compassionate care, however, is a skill set that has dwindled from the field of ABA in recent years. The Clinician’s Toolbox: RediscoveringCompassionate ABAreminds practitioners just how important compassion is to their practice.
With tools for navigating the landscape of ABA as it exists today, The Clinician’s Toolbox explores the range of skill sets that make up compassionate care—with patients, parents, and other practitioners. Making compassion clear and actionable, The Clinician’s Toolbox is a valuable guide for practitioners at any stage in their career seeking to expand their understanding and practice of compassionate care.
About the Authors
Dr. Ronald Leaf is a licensed psychologist with over 45 years of experience in the field of autism. Dr. Leaf began his career working with Professor Ivar Lovaas, while receiving his undergraduate degree at University of California, Los Angeles (UCLA). Subsequently, he received his doctorate under the direction of Prof. Lovaas. During his years at UCLA, he served as Clinic Supervisor, Research Psychologist, Lecturer and Interim Director of the Young Autism Project. He was extensively involved in several research investigations, contributed to The Me Book, and is a co-author of The Me Book Videotapes. Dr. Leaf has consulted to families, schools, and agencies on a national and international basis. He is the Co-founder and Director of Autism Partnership, which offers comprehensive services for families with children and adolescents diagnosed with autism spectrum disorder (ASD). With offices in 10 countries, Ron and his team have developed the Autism Partnership Method, a progressive approach to implementing Applied Behavior Analysis (ABA) treatment. He is co-author of A Work in Progress, Time for School, It Has to Be Said, Crafting Connections, A Work in Progress Companion Series, Clinical Judgment and Autism Partnership Method: Social Skill Group. He has co-authored over 75 articles in research journals and presented over 100 times at professional conferences. Dr. Leaf is also the co-founder of the Autism Partnership Foundation, a non-profit dedicated to advancing professional standards and treatment of individuals with autism through research and training.
Jamison Dayharsh is a licensed Marriage and Family Therapist. Ms. Dayharsh began working with children with autism spectrum disorder in the late 1970s at UCLA on the Young Autism Project, where she served as a Senior Therapist, Research Assistant, and Teaching Assistant. She earned her master’s degree in counseling psychology at Loyola Marymount University in 1983. Ms. Dayharsh is the Executive Director of Behavior Therapy and Learning Center. Her work has included parent training and consulting nationally and internationally to parents, schools and mental health agencies. Ms. Dayharsh is an author of A Work in Progress, a book on behavioral treatment and a contributor to research publications. Ms. Dayharsh’s expertise includes counseling families of children with disabilities as well as providing psychotherapy to children and adolescents with autism spectrum disorders.
Jonathan Rafuse is a Board-Certified Behavior Analyst who graduated from UCLA in 1988 with a bachelor’s degree in psychology. In 1991, he received his master’s degree in clinical psychology from Antioch University. He furthered his graduate studies in 2017, completing coursework at the University of North Texas. During his master’s coursework he was the Clinical Director for 1736 Family Crisis Center’s Youth Shelter, overseeing the intense therapy and treatment provided to runaway and abused adolescents. In 1992, he began work at the May Institute running an off-campus group home serving students dramatically impacted with ASD. In 1995, he joined Autism Partnership, which offers comprehensive services for families with children and adolescents with autism spectrum disorder (ASD), and where he is a Clinical Director. He oversees the clinical and programmatic direction of therapy teams providing treatment to this highly individualized population. His responsibilities further include advanced training, mentoring, and consultation to ABA-service providers and teaching staff within school districts and private agencies across the country. He has presented both nationally and internationally at conferences on Applied Behavior Analysis, and consults throughout the United States, Australia and Asia. He wrote chapters in Crafting Connections and The Autism Partnership Method: Social Skills Groups and contributed to the video companion series to A Work in Progress.
John McEachin, a Licensed Psychologist, Licensed Behavior Analyst, and Progressive Behavior Analyst-Autism Professional, has been providing behavioral services and conducting research on autism for five decades. He received his graduate training under Professor Ivar Lovaas at UCLA on the Young Autism Project. During his 11 years at UCLA, Dr. McEachin served in various roles including Clinic Supervisor, Research and Teaching Assistant, and Instructor. His research has included the long-term follow-up study of young autistic children who received intensive behavioral treatment, which was published in 1993. In 1994 he joined with Ron Leaf in forming Autism Partnership, which they co-direct. In 1999 they published A Work in Progress, a widely used behavioral treatment manual and curriculum for children with ASD. Dr. McEachin has lectured throughout the world and co-authored several books and more than 100 research articles published in peer reviewed journals. Besides his clinical and research work, he is currently President of the Progressive Behavior Analyst Autism Council and an instructor in the Psychology department at Long Beach State University.
Justin Leaf, Ph.D., is the Executive Director for Autism Partnership Foundation and the Progressive Behavior Analyst Autism Council, the Associate Director for ABA Doctoral Studies at Endicott College, and the Executive Director for Contemporary Behavior Consultants. Dr. Leaf received his doctorate degree in Behavioral Psychology from the Department of Applied Behavioral Science at the University of Kansas. His research interests include Progressive ABA, improving behavioral intervention, social behavior, and methodologies to improve the lives of autistic/individuals diagnosed with ASD. He has over 140 publications in either peer reviewed journals, books, or book chapters and has presented at both national and international professional conferences and invited events. He has served on numerous editorial boards for behavior analytic and autism journals. Justin career has been dedicated to improving the field of Applied Behavior Analysis and lives of individuals with autism.